

A contemporary European experience with surgical septal myectomy in hypertrophic cardiomyopathy
- PMID: 22522842
- PMCID: PMC3418509
- DOI: 10.1093/eurheartj/ehs064
A contemporary European experience with surgical septal myectomy in hypertrophic cardiomyopathy
Abstract
Aims: The recent American College of Cardiology and American Heart Association Guidelines on hypertrophic cardiomyopathy (HCM) have confirmed surgical myectomy as the gold standard for non-pharmacological treatment of obstructive HCM. However, during the last 15 years, an extensive use of alcohol septal ablation has led to the virtual extinction of myectomy programmes in several European countries. Therefore, many HCM candidates for myectomy in Europe cannot be offered the option of this procedure. The purpose of our study is to report the difficulties and results in developing a myectomy programme for HCM in a centre without previous experience with this procedure.
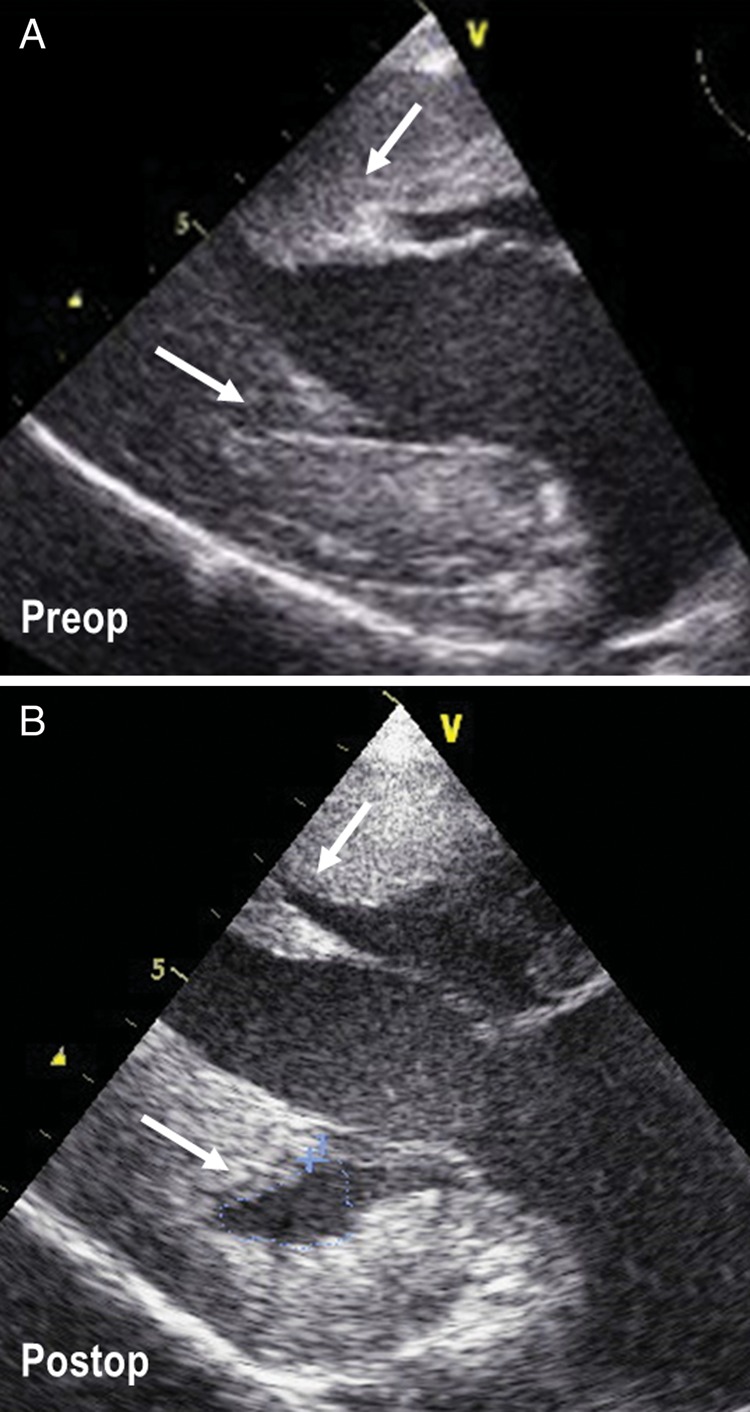
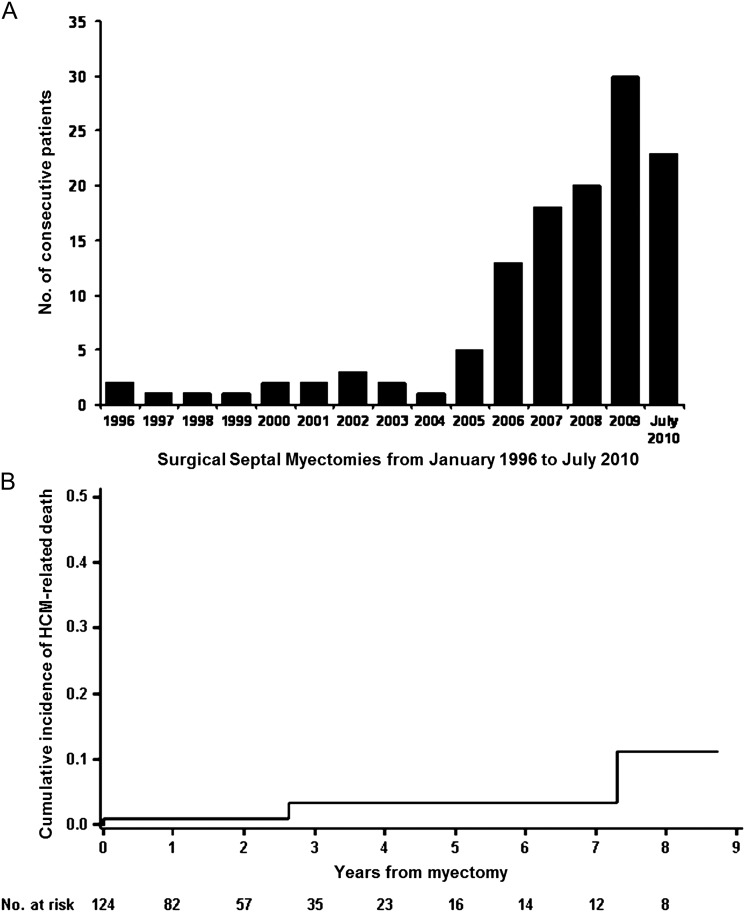
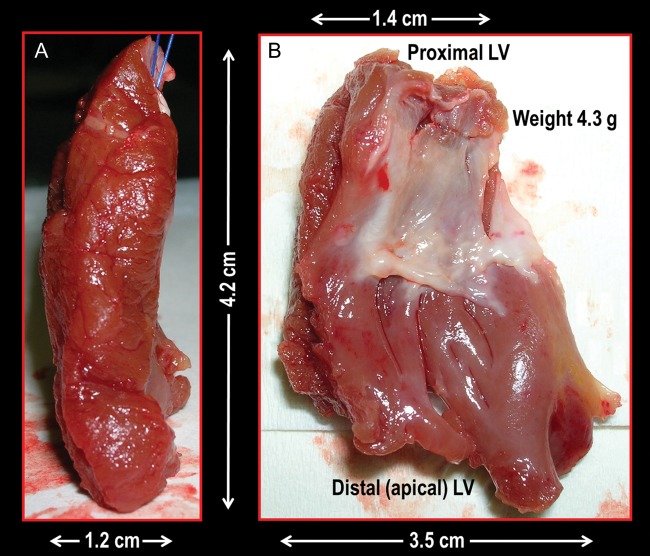
Methods and results: The clinical course is reported of 124 consecutive patients with obstructive HCM and heart failure symptoms who underwent myectomy at a single European centre between 1996 and 2010. The median follow-up was 20.3 months (inter-quartile range: 3.9-40.6 months). No patients were lost to follow-up. A cumulative incidence of HCM-related death after myectomy was 0.8, 3.3, and 11.2% at 1, 5, and 10 years, respectively, including one operative death (procedural mortality 0.8%). The left ventricular (LV) outflow gradient decreased from 95 ± 36 mmHg before surgery to 12 ± 6 mmHg at most recent evaluation (P < 0.001), with none of the patients having a significant residual LV outflow gradient. Of the 97 patients in New York Heart Association functional class III-IV before surgery, 93 (96%) were in class I-II at most recent evaluation (P < 0.001).
Conclusion: Our results show that the development of a myectomy programme at a centre without previous experience with this procedure is feasible and can lead to highly favourable clinical results.
Figures
Comment in
-
Septal myectomy remains the gold standard.Eur Heart J. 2012 Aug;33(16):1999-2000. doi: 10.1093/eurheartj/ehs125. Epub 2012 Jun 26. Eur Heart J. 2012. PMID: 22736677 No abstract available.
References
-
- Maron BJ, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn HJ, Seidman CE, Shah PM, Spencer WH, III, Spirito P, Ten Cate FJ, Wigle ED. American College of Cardiology/European Society of Cardiology Clinical Expert Consensus Document on Hypertrophic Cardiomyopathy. A report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents and the European Society of Cardiology Committee for Practice Guidelines. J Am Coll Cardiol. 2003;42:1687–1713. - PubMed
-
- Gersh BJ, Maron BJ, Bonow RO, Dearani JA, Fifer MA, Link MS, Naidu SS, Nishimura RA, Ommen SR, Rakowski H, Seidman CE, Towbin JA, Udelson JE, Yancy CW. 2011 ACCF/AHA Guideline for the Diagnosis and Treatment of Hypertrophic Cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2011;58:e212–e260. - PubMed
-
- Sigwart U. Non-surgical myocardial reduction for hypertrophic obstructive cardiomyopathy. Lancet. 1995;346:211–214. - PubMed
-
- Faber L, Seggewiss H, Gleichmann U. Percutaneous transluminal septal myocardial ablation in hypertrophic obstructive cardiomyopathy: results with respect to intraprocedural myocardial contrast echocardiography. Circulation. 1998;98:2415–2421. - PubMed
-
- Henein MY, O'Sullivan CA, Ramzy IS, Sigwart U, Gibson DG. Electromechanical left ventricular behavior after nonsurgical septal reduction in patients with hypertrophic obstructive cardiomyopathy. J Am Coll Cardiol. 1999;34:1117–1122. - PubMed
