

Clinically concordant variations of Alzheimer pathology in aphasic versus amnestic dementia
- PMID: 22522938
- PMCID: PMC3338929
- DOI: 10.1093/brain/aws076
Clinically concordant variations of Alzheimer pathology in aphasic versus amnestic dementia
Abstract
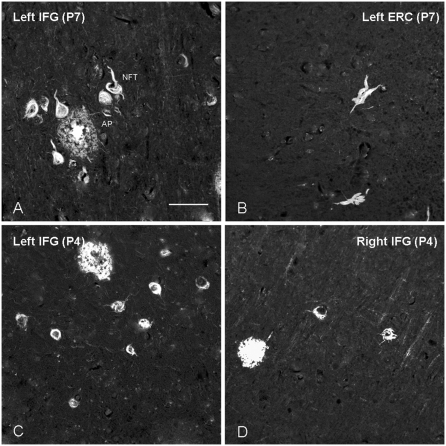
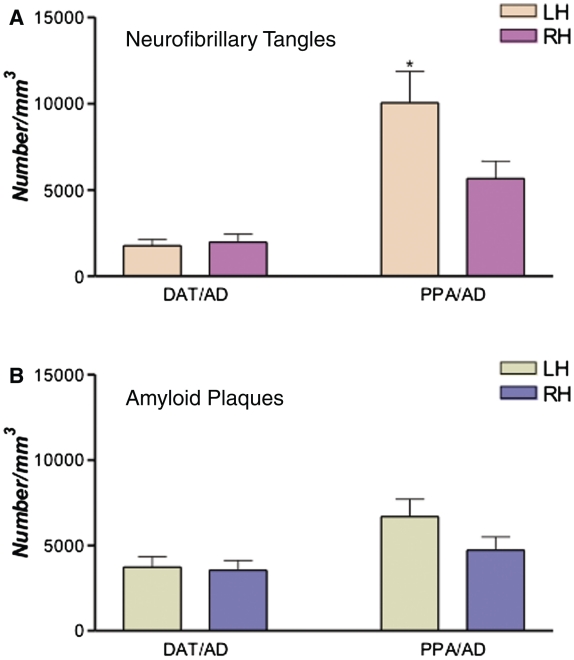
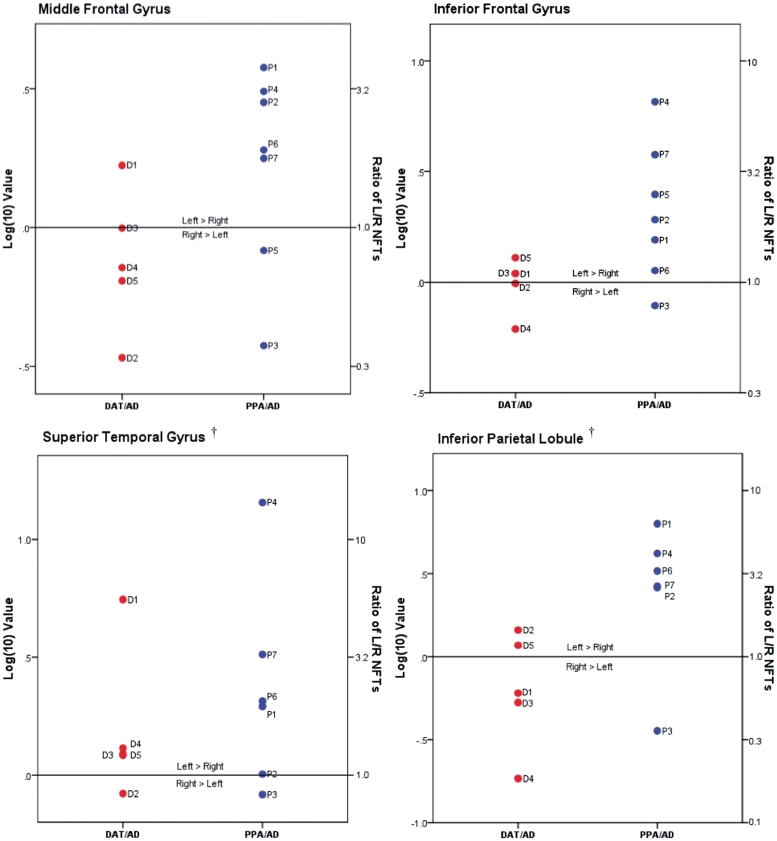
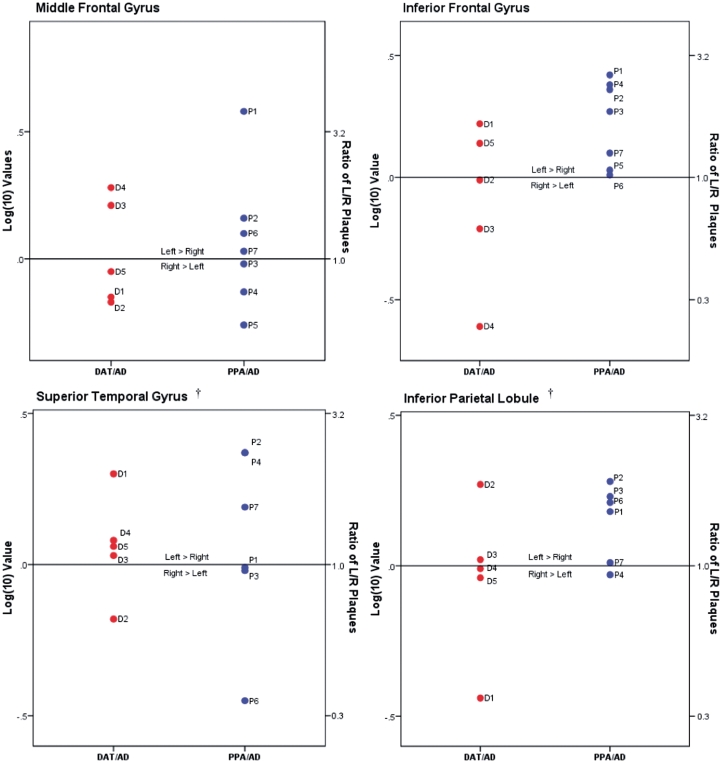
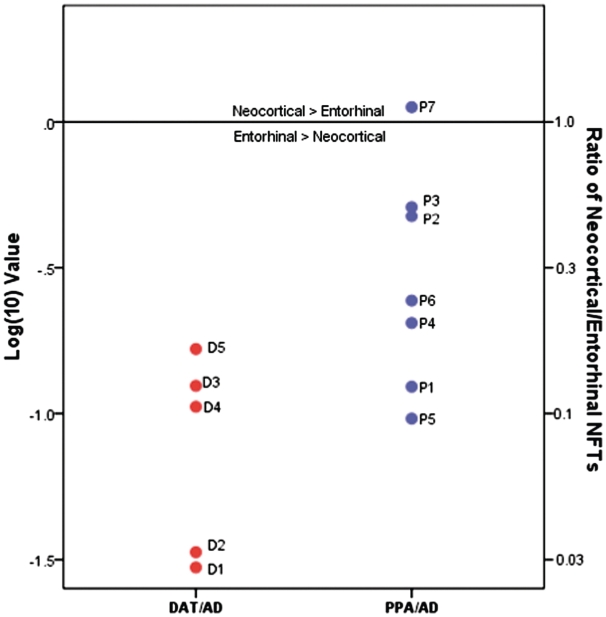
Primary progressive aphasia is a neurodegenerative syndrome characterized by gradual dissolution of language but relative sparing of other cognitive domains, especially memory. It is associated with asymmetric atrophy in the language-dominant hemisphere (usually left), and differs from typical Alzheimer-type dementia where amnesia is the primary deficit. Various pathologies have been reported, including the tangles and plaques of Alzheimer's disease. Identification of Alzheimer pathology in these aphasic patients is puzzling since tangles and related neuronal loss in Alzheimer's disease typically emerge in memory-related structures such as entorhinal cortex and spread to language-related neocortex later in the disease. Furthermore, Alzheimer pathology is typically symmetric. How can a predominantly limbic and symmetric pathology cause the primary progressive aphasia phenotype, characterized by relative preservation of memory and asymmetric predilection for the language-dominant hemisphere? Initial investigations into the possibility that Alzheimer pathology displays an atypical distribution in primary progressive aphasia yielded inconclusive results. The current study was based on larger groups of patients with either primary progressive aphasia or a typical amnestic dementia. Alzheimer pathology was the principal diagnosis in all cases. The goal was to determine whether Alzheimer pathology had clinically-concordant, and hence different distributions in these two phenotypes. Stereological counts of tangles and plaques revealed greater leftward asymmetry for tangles in primary progressive aphasia but not in the amnestic Alzheimer-type dementia (P < 0.05). Five of seven aphasics had more leftward tangle asymmetry in all four neocortical regions analysed, whereas this pattern was not seen in any of the predominantly amnestic cases. One aphasic case displayed higher right-hemisphere tangle density despite greater left-hemisphere hypoperfusion and atrophy during life. Although there were more tangles in the memory-related entorhinal cortex than in language-related neocortical areas in both phenotypes (P < 0.0001), the ratio of neocortical-to-entorhinal tangles was significantly higher in the aphasic cases (P = 0.034). Additionally, overall numbers of tangles and plaques were greater in the aphasic than amnestic cases (P < 0.05), especially in neocortical areas. No significant hemispheric asymmetry was found in plaque distribution, reinforcing the conclusion that tangles have greater clinical concordance than plaques in the spectrum of Alzheimer pathologies. The presence of left-sided tangle predominance and higher neocortical-to-entorhinal tangle ratio in primary progressive aphasia establishes clinical concordance of Alzheimer pathology with the aphasic phenotype. The one case with reversed asymmetry, however, suggests that these concordant clinicopathological relationships are not universal and that individual primary progressive aphasia cases with Alzheimer pathology exist where distributions of plaques and tangles do not account for the observed phenotype.
Figures

References
-
- Arriagada PV, Growdon JH, Hedley-Whyte T, Hyman BT. Neurofibrillary tangles but not senile plaques parallel duration and severity of Alzheimer's disease. Neurology. 1992;42(Pt 1):631–9. - PubMed
-
- Benson DF, Davis RJ, Snyder BD. Posterior cortical atrophy. Arch Neurol. 1988;45:789–93. - PubMed
-
- Bierer LM, Hof PR, Purohit DP, Carlin L, Schmeidler J, Davis KL, et al. Neocortical neurofibrillary tangles correlate with dementia severity in Alzheimer's disease. Arch Neurol. 1995;52:81–8. - PubMed
-
- Bobinski M, Wegiel J, Wisniewski HM, Tarnawski M. Neurofibrillary pathology—correlation with hippocampal formation atrophy in Alzheimer disease. Neurobiol Aging. 1996;17:909–19. - PubMed
-
- Braak H, Braak E. Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol. 1991;82:239–59. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
