

Blood pressure change in normotensive, gestational hypertensive, preeclamptic, and essential hypertensive pregnancies
- PMID: 22526257
- PMCID: PMC3378662
- DOI: 10.1161/HYPERTENSIONAHA.111.187039
Blood pressure change in normotensive, gestational hypertensive, preeclamptic, and essential hypertensive pregnancies
Abstract
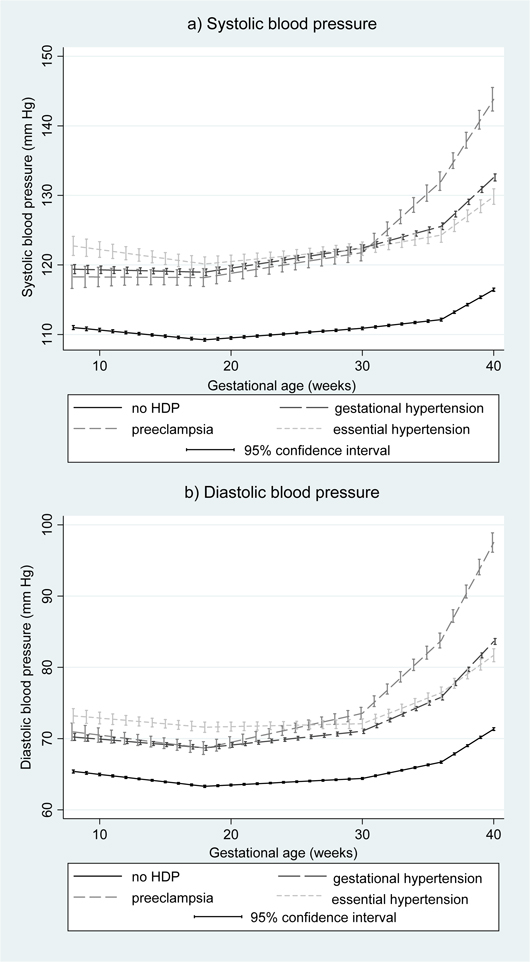
We compared patterns of blood pressure (BP) change among normotensive women, women who developed gestational hypertension or preeclampsia, and women who had essential hypertension to examine how distinct these conditions are and whether rates of BP change may help to identify women at risk for hypertensive disorders. We used antenatal clinic BP measurements (median, 14 per woman) of 13016 women from the Avon Longitudinal Study of Parents and Children who had a singleton or twin live birth surviving until ≥ 1 year. Linear spline models were used to describe changes in systolic and diastolic BPs in different periods of pregnancy (8-18, 18-30, 30-36, and ≥ 36 weeks' gestation). Women who had essential hypertension and those who developed gestational hypertension or preeclampsia had higher BP at 8 weeks' gestation (baseline) compared with normotensive women. The decrease in BP until 18 weeks was smaller in gestational hypertensive compared with normotensive pregnancies. BP rose more rapidly from 18 weeks onward in gestational hypertensive and preeclamptic pregnancies and from 30 weeks onward in essential hypertensive compared with normotensive pregnancies. Women who developed preeclampsia had a more rapid increase in BP from 30 weeks onward than those who developed gestational hypertension or had essential hypertension. Our findings indicate notable patterns of BP change that distinguish women with essential hypertension, gestational hypertension, and preeclampsia from each other and from normotensive women, even from early pregnancy. These distinct patterns may be useful for identifying women at risk of developing a hypertensive disorder later in pregnancy.
Figures
Comment in
-
Preeclampsia: the role of aldosterone in hypertension and inflammation.Hypertension. 2012 Jun;59(6):1099-100. doi: 10.1161/HYPERTENSIONAHA.112.193011. Epub 2012 Apr 23. Hypertension. 2012. PMID: 22526256 No abstract available.
References
-
- Roberts CL, Algert CS, Morris JM, Ford JB, Henderson-Smart DJ. Hypertensive disorders in pregnancy: a population-based study. Med J Australia. 2005;182:332–335. - PubMed
-
- The Confidential Enquiry into Maternal and Child Health (CEMACH) In: Saving Mothers’ Lives: Reviewing Maternal Deaths to Make Motherhood Safer-2003-2005. Lewis G, editor. The Seventh Report on Confidential Enquiries into Maternal Deaths in the United Kingdom; 2007.
-
- Steegers EA, von DP, Duvekot JJ, Pijnenborg R. Pre-eclampsia. Lancet. 2010;376:631–644. - PubMed
-
- Buchbinder A, Sibai BM, Caritis S, MacPherson C, Hauth J, Lindheimer MD, Klebanoff M, VanDorsten P, Landon M, Paul R, Miodovnik M, Meis P, Thurnau G. Adverse perinatal outcomes are significantly higher in severe gestational hypertension than in mild preeclampsia. Am J Obstet Gynecol. 2002;186:66–71. - PubMed
-
- Heard AR, Dekker GA, Chan A, Jacobs DJ, Vreeburg SA, Priest KR. Hypertension during pregnancy in South Australia, Part 1: Pregnancy outcomes. Aust NZ J Obstet Gyn. 2004;44:404–409. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
