

In-line filtration reduces severe complications and length of stay on pediatric intensive care unit: a prospective, randomized, controlled trial
- PMID: 22527062
- PMCID: PMC3351606
- DOI: 10.1007/s00134-012-2539-7
In-line filtration reduces severe complications and length of stay on pediatric intensive care unit: a prospective, randomized, controlled trial
Abstract
Purpose: Particulate contamination due to infusion therapy carries a potential health risk for intensive care patients.
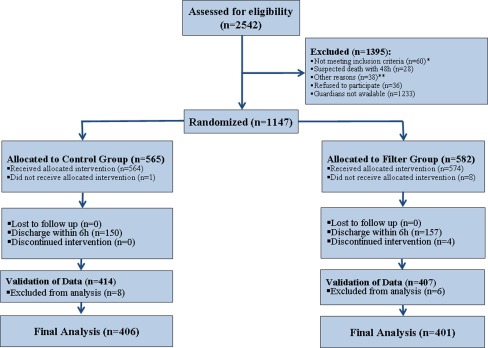
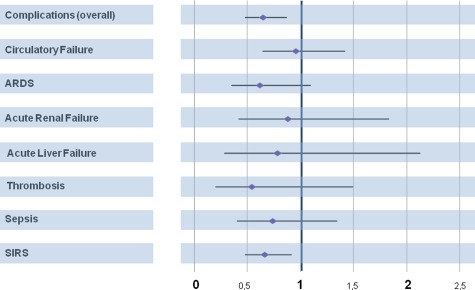
Methods: This single-centre, prospective, randomized controlled trial assessed the effects of filtration of intravenous fluids on the reduction of complications in critically ill children admitted to a pediatric intensive care unit (PICU). A total of 807 subjects were randomly assigned to either a control (n = 406) or filter group (n = 401), with the latter receiving in-line filtration. The primary endpoint was reduction in the rate of overall complications, which included the occurrence of systemic inflammatory response syndrome (SIRS), sepsis, organ failure (circulation, lung, liver, kidney) and thrombosis. Secondary objectives were a reduction in the length of stay on the PICU and overall hospital stay. Duration of mechanical ventilation and mortality were also analyzed.
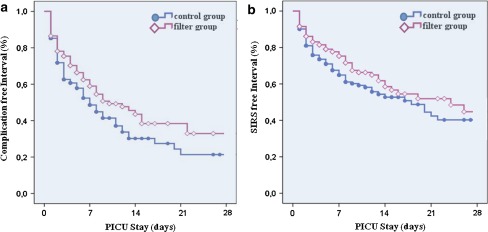
Findings: Analysis demonstrated a significant reduction in the overall complication rate (n = 166 [40.9 %] vs. n = 124 [30.9 %]; P = 0.003) for the filter group. In particular, the incidence of SIRS was significantly lower (n = 123 [30.3 %] vs. n = 90 [22.4 %]; P = 0.01). Moreover the length of stay on PICU (3.89 [95 % confidence interval 2.97-4.82] vs. 2.98 [2.33-3.64]; P = 0.025) and duration of mechanical ventilation (14.0 [5.6-22.4] vs. 11.0 [7.1-14.9] h; P = 0.028) were significantly reduced.
Conclusion: In-line filtration is able to avert severe complications in critically ill patients. The overall complication rate during the PICU stay among the filter group was significantly reduced. In-line filtration was effective in reducing the occurrence of SIRS. We therefore conclude that in-line filtration improves the safety of intensive care therapy and represents a preventive strategy that results in a significant reduction of the length of stay in the PICU and duration of mechanical ventilation (ClinicalTrials.gov number: NCT00209768).
Figures
References
-
- Hellinger A, Piotrowski J, Konerding MA, Burchard WG, Doetsch N, Peitgen K, Erhard J, Reidemeister JC. Impact of particulate contamination in crystalloid cardioplegic solutions: studies by scanning and transmission electron microscopy. Thorac Cardiovasc Surg. 1997;45:20–26. doi: 10.1055/s-2007-1013678. - DOI - PubMed
-
- Schroder F. Compatibility problems in intensive care medicine. Infusionsther Transfusionsmed. 1994;21:52–58. - PubMed
-
- Ball PA. Intravenous in-line filters: filtering the evidence. Curr Opin Clin Nutr Metab Care. 2003;6:319–325. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
