

Therapeutic strategies for bone metastases and their clinical sequelae in prostate cancer
- PMID: 22528368
- PMCID: PMC3652976
- DOI: 10.1007/s11864-012-0190-8
Therapeutic strategies for bone metastases and their clinical sequelae in prostate cancer
Abstract
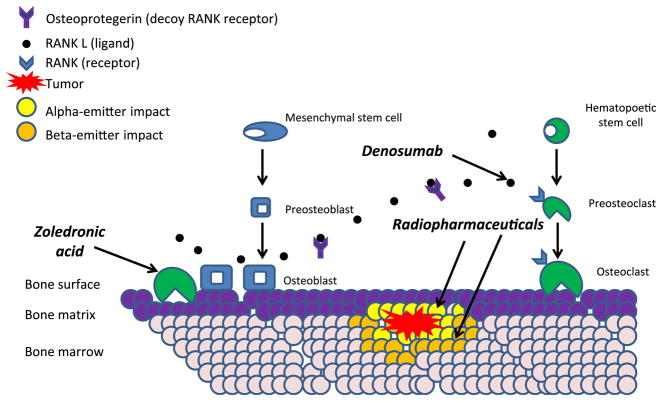
Skeletal metastases threaten quality of life, functionality, and longevity in patients with metastatic castration-resistant prostate cancer (mCRPC). Therapeutic strategies for bone metastases in prostate cancer can palliate pain, delay/prevent skeletal complications, and prolong survival. Pharmacologic agents representing several drug classes have demonstrated the ability to achieve these treatment goals in men with mCRPC. Skeletal-related events such as fracture and the need for radiation can be delayed using drugs that target the osteoclast/osteoblast pathway. Cancer-related bone pain can be palliated using beta-emitting bone-seeking radiopharmaceuticals such as samarium-153 EDTMP and strontium-89. Also, prospective randomized studies have demonstrated that cytotoxic chemotherapy can palliate bone pain. For the first time, bone-directed therapy has been shown to prolong survival using the novel alpha-emitting radiopharmaceutical radium-223. Given these multifold clinical benefits, treatments targeting bone metabolism, tumor-bone stromal interactions, and bone metastases themselves are now central elements of routine clinical care. Decisions about which agents, alone or in combination, will best serve the patient's and clinician's clinical goals is contingent on the treatment history to date, present disease manifestations, and symptomatology. Clinical trials exploring novel agents such as those targeting c-Met and Src are under way, using endpoints that directly address how patients feel, function, and survive.
Figures
References
-
- Coleman R. Management of bone metastases. Cancer Treat Rev. 1997;23 (Suppl 1):S69–75. - PubMed
-
- Fizazi K, Beuzeboc P, Lumbroso J, et al. Phase II trial of consolidation docetaxel and samarium-153 in patients with bone metastases from castration-resistant prostate cancer. J Clin Oncol. 2009;27 (15):2429–35. - PubMed
-
- Saad F, Olsson C, Schulman CC. Skeletal morbidity in men with prostate cancer: quality-of-life considerations throughout the continuum of care. Eur Urol. 2004;46(6):731–39. discussion 739–40. - PubMed
-
- Fizazi K, Carducci M, Smith M, et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind study. Lancet. 2011;377(9768):813–22. This large, randomized, non-inferiority trial demonstrated that denosumab delayed skeletal-related events by 3.6 months relative to zoledronic acid in men with mCRPC. Both agents are FDA approved to delay skeletal events in metastatic castration-resistant disease. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
