

Does augmentation with a reinforced fascia patch improve rotator cuff repair outcomes?
- PMID: 22528381
- PMCID: PMC3830110
- DOI: 10.1007/s11999-012-2348-x
Does augmentation with a reinforced fascia patch improve rotator cuff repair outcomes?
Abstract
Background: Scaffold devices are used to augment rotator cuff repairs in humans. While the strength of a novel poly-L-lactic acid-reinforced (human) fascia patch has been documented, it is unclear whether such patches will enhance the strength or likelihood of healing of rotator cuff repairs.
Questions/purposes: In a canine shoulder model, we asked: Do tendon repairs augmented with a reinforced fascia patch have (1) increased biomechanical properties at Time 0 and (2) less tendon retraction and increased cross-sectional area and biomechanical properties after 12 weeks of healing compared to repairs without augmentation? (3) Do the biomechanical properties of tendon repairs reach normal values by 12 weeks of healing? And (4) is the host response associated with use of the reinforced fascia patch biocompatible?
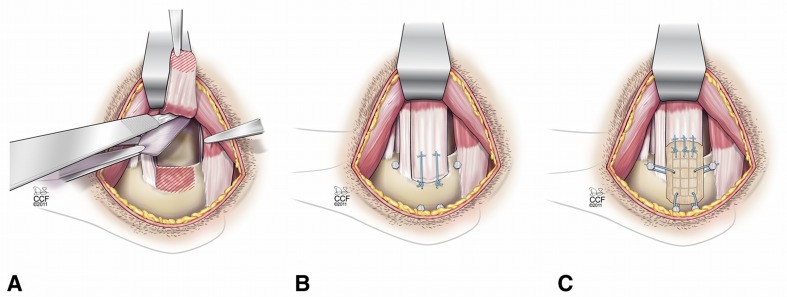
Methods: Eleven dogs underwent bilateral shoulder surgery with partial release and acute repair of the infraspinatus tendon, one shoulder with augmentation and one without augmentation. Repair retraction, cross-sectional area, biomechanical properties, and biocompatibility were assessed at 12 weeks.
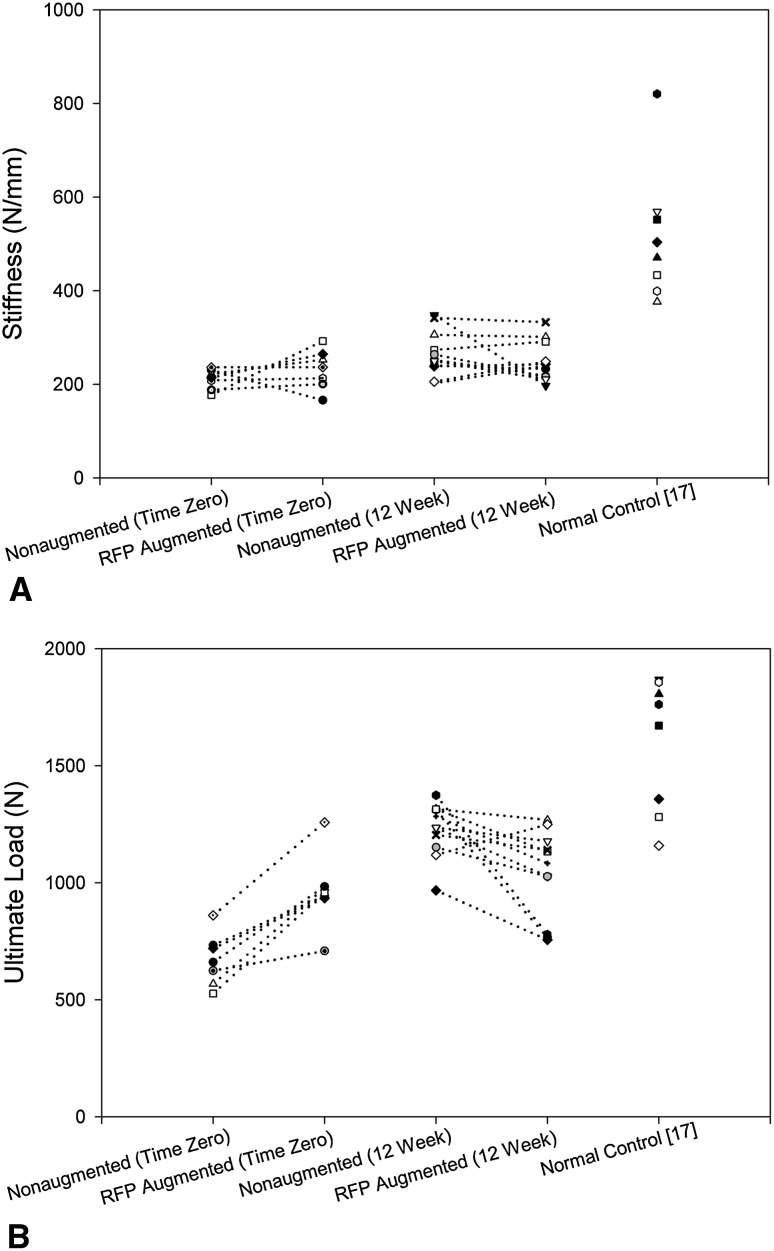
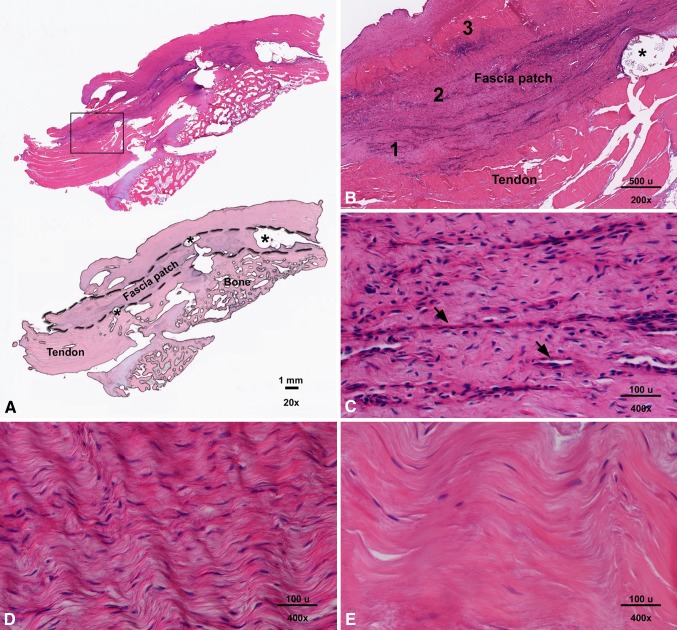
Results: At Time 0, the mean ± SD ultimate load of augmented repairs was 296 ± 130 N (46% ± 25%) more than nonaugmented repairs, with no difference in stiffness between groups. At 12 weeks, the ultimate load of augmented repairs averaged 192 ± 213 N (15% ± 16%) less than nonaugmented repairs, with no difference in stiffness between groups. At the tendon repair site at 12 weeks, the fascia patch showed a biocompatible host tissue response.
Conclusions: The biomechanical properties of repairs augmented with a reinforced fascia patch demonstrated greater ultimate load at Time 0 than nonaugmented repairs but remained essentially unchanged after 12 weeks of healing, despite improvements in the ultimate load of nonaugmented controls in the same time frame.
Figures
References
-
- Accousti KJ, Flatow EL. Technical pearls on how to maximize healing of the rotator cuff. Instr Course Lect. 2007;56:3–12. - PubMed
-
- Aurora A, Mesiha M, Tan CD, Walker E, Sahoo S, Iannotti JP, McCarron JA, Derwin KA. Mechanical characterization and biocompatibility of a novel reinforced fascia patch for rotator cuff repair. J Biomed Mater Res A. 2011;99:221–230. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
