

The power of the National Surgical Quality Improvement Program--achieving a zero pneumonia rate in general surgery patients
- PMID: 22529758
- PMCID: PMC3327110
- DOI: 10.7812/TPP/11-127
The power of the National Surgical Quality Improvement Program--achieving a zero pneumonia rate in general surgery patients
Abstract
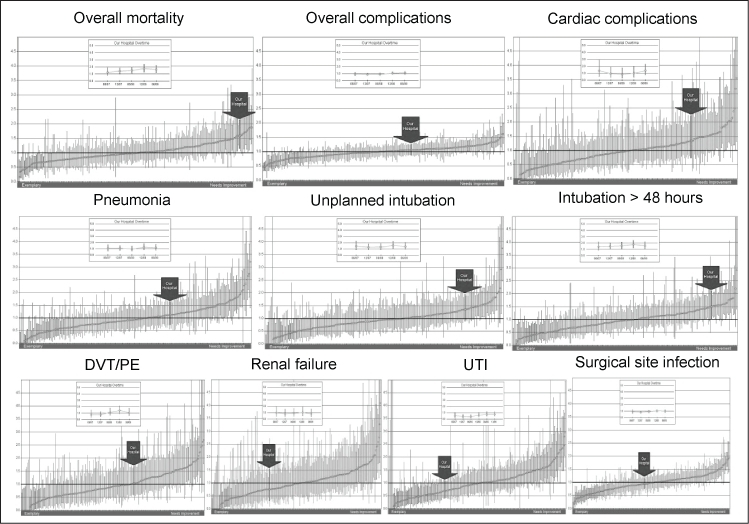
The National Surgical Quality Improvement Program (NSQIP) of the American College of Surgeons provides risk-adjusted surgical outcome measures for participating hospitals that can be used for performance improvement of surgical mortality and morbidity. A surgical clinical nurse reviewer collects 135 clinical variables including preoperative risk factors, intraoperative variables, and 30-day postoperative mortality and morbidity outcomes for patients undergoing major surgical procedures. A report on mortality and complications is prepared twice a year. This article summarizes briefly the history of NSQIP and how its report on surgical outcomes can be used for performance improvement within a hospital system. In particular, it describes how to drive performance improvement with NSQIP data using the example of postoperative respiratory complications--a major factor of postoperative mortality. In addition, this article explains the benefit of a collaborative of several participating NSQIP hospitals and describes how to develop a "playbook" on the basis of an outcome improvement project.
Figures










References
-
- National Surgical Quality Improvement Program [home page on the Internet] Chicago, IL: American College of Surgeons; 2005. [cited 2012 Jan 17]. Available from: www.acsnsqip.org.
-
- Ingraham AM, Richards KE, Hall BL, Ko CY. Quality improvement in surgery: the American College of Surgeons National Surgical Quality Improvement Program approach. Adv Surg. 2010;(44):251–67. - PubMed
-
- Veterans' Administration Health-Care Amendments of 1985, Pub L No 99–166, 99 Stat 941. Dec 3, 1985. Title II: Health-Care Administration, Sec. 201– 4.
-
- Khuri SF, Daley J, Henderson WG. The comparative assessment and improvement of quality of surgical care in the Department of Veterans Affairs. Arch Surg. 2002 Jan;137(1):20–7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
