

A population-based study of human papillomavirus genotype prevalence in the United States: baseline measures prior to mass human papillomavirus vaccination
- PMID: 22532127
- PMCID: PMC3852415
- DOI: 10.1002/ijc.27608
A population-based study of human papillomavirus genotype prevalence in the United States: baseline measures prior to mass human papillomavirus vaccination
Abstract
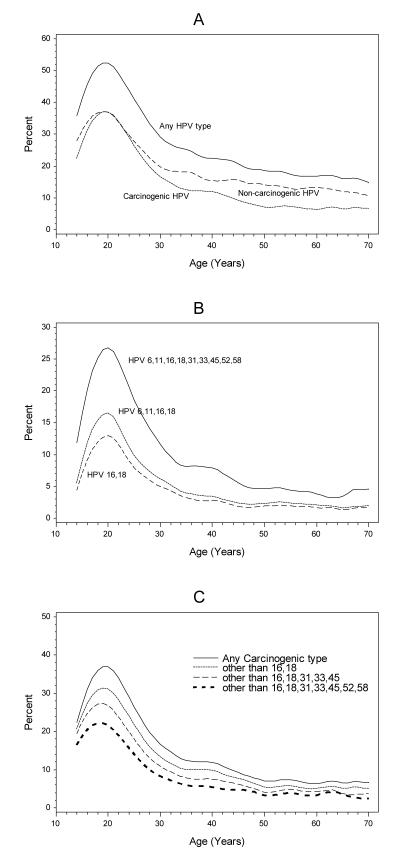
Currently, two prophylactic human papillomavirus (HPV) vaccines targeting HPV 16 and 18 have been shown to be highly efficacious for preventing precursor lesions although the effectiveness of these vaccines in real-world clinical settings must still be determined. Toward this end, an ongoing statewide surveillance program was established in New Mexico to assess all aspects of cervical cancer preventive care. Given that the reduction in cervical cancer incidence is expected to take several decades to manifest, a systematic population-based measurement of HPV type-specific prevalence employing an age- and cytology-stratified sample of 47,617 women attending for cervical screening was conducted prior to widespread HPV vaccination. A well-validated polymerase chain reaction (PCR) method for 37 HPV genotypes was used to test liquid-based cytology specimens. The prevalence for any of the 37 HPV types was 27.3% overall with a maximum of 52% at age of 20 years followed by a rapid decline at older ages. The HPV 16 prevalences in women aged ≤ 20 years, 21-29 years or ≥ 30 years were 9.6, 6.5 and 1.8%, respectively. The combined prevalences of HPV 16 and 18 in these age groups were 12.0, 8.3 and 2.4%, respectively. HPV 16 and/or HPV 18 were detected in 54.5% of high-grade squamous intraepithelial (cytologic) lesions (HSIL) and in 25.0% of those with low-grade SIL (LSIL). These baseline data enable estimates of maximum HPV vaccine impact across time and provide critical reference measurements important to assessing clinical benefits and potential harms of HPV vaccination including increases in nonvaccine HPV types (i.e., type replacement).
Copyright © 2012 UICC.
Figures
References
-
- Walboomers JM, Jacobs MV, Manos MM, Bosch FX, Kummer JA, Shah KV, Snijders PJ, Peto J, Meijer CJ, Muñoz N. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol. 1999;189:12–19. - PubMed
-
- Mayrand MH, Duarte-Franco E, Rodrigues I, Walter SD, Hanley J, Ferenczy A, Ratnam S, Coutlée F, Franco EL, Canadian Cervical Cancer Screening Trial Study Group Human papillomavirus DNA versus Papanicolaou screening tests for cervical cancer. N Engl J Med. 2007;357:1579–1588. - PubMed
-
- Naucler P, Ryd W, Tornberg S, Strand A, Wadell G, Elfgren K, Rådberg T, Strander B, Forslund O, Hansson BG, Hagmar B, Johansson B, et al. Human papillomavirus and Papanicolaou tests to screen for cervical cancer. N Engl J Med. 2007;357:1589–1597. - PubMed
-
- Bulkmans NW, Berkhof J, Rozendaal L, van Kemenade FJ, Boeke AJ, Bulk S, Voorhorst FJ, Verheijen RH, van Groningen K, Boon ME, Ruitinga W, van Ballegooijen M, et al. Human papillomavirus DNA testing for the detection of cervical intraepithelial neoplasia grade 3 and cancer: 5-year follow-up of a randomised controlled implementation trial. Lancet. 2007;370:1764–1772. - PubMed
