

Safety in glomerular numbers
- PMID: 22532329
- PMCID: PMC3422453
- DOI: 10.1007/s00467-012-2169-x
Safety in glomerular numbers
Abstract
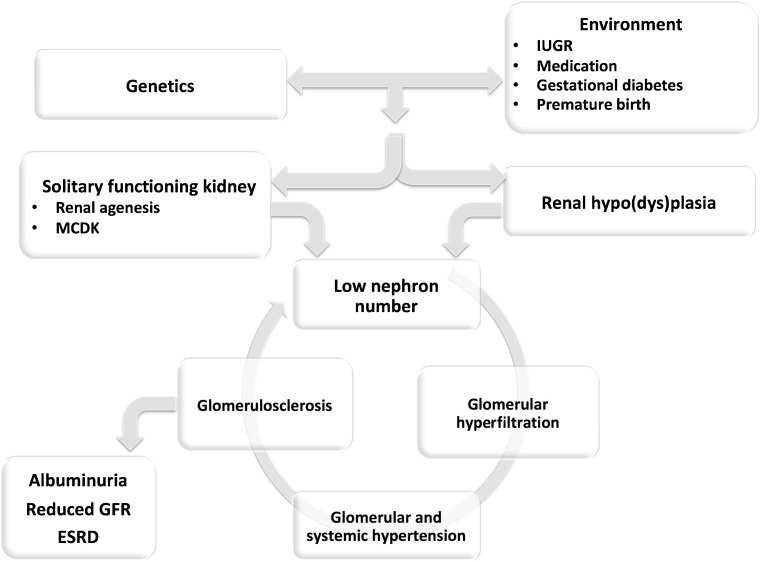
A low nephron number is, according to Brenner's hyperfiltration hypothesis, associated with hypertension, glomerular damage and proteinuria, and starts a vicious cycle that ends in renal failure over the long term. Nephron endowment is set during foetal life, and there is no formation of nephrons after 34-36 weeks of gestation, indicating that many factors before that time-point may have an impact on kidney development and reduce nephron numbers. Such factors include maternal malnutrition, stress, diseases, such as diabetes, uteroplacental insufficiency, maternal and neonatal drugs and premature birth. However, other congenital anomalies, such as renal hypoplasia, unilateral renal agenesis or multicystic dysplastic kidney, may also lead to a reduced nephron endowment, with an increased risk for hypertension, renal dysfunction and the need for renal replacement therapy. This review focuses on the causes and consequences of a low nephron endowment and will illustrate why there is safety in glomerular numbers.
Figures
Comment in
-
Re: Safety in glomerular numbers.Pediatr Nephrol. 2013 Aug;28(8):1319. doi: 10.1007/s00467-013-2442-7. Epub 2013 Mar 26. Pediatr Nephrol. 2013. PMID: 23529639 No abstract available.
References
-
- Brenner BM. Brenner and Rector's the kidney. 8th. Philadelphia: Saunders, Elsevier; 2008. pp. 3–24.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
