

Discrimination of ischemic and hemorrhagic strokes using a multiplexed, mass spectrometry-based assay for serum apolipoproteins coupled to multi-marker ROC algorithm
- PMID: 22532455
- PMCID: PMC3910141
- DOI: 10.1002/prca.201100041
Discrimination of ischemic and hemorrhagic strokes using a multiplexed, mass spectrometry-based assay for serum apolipoproteins coupled to multi-marker ROC algorithm
Abstract
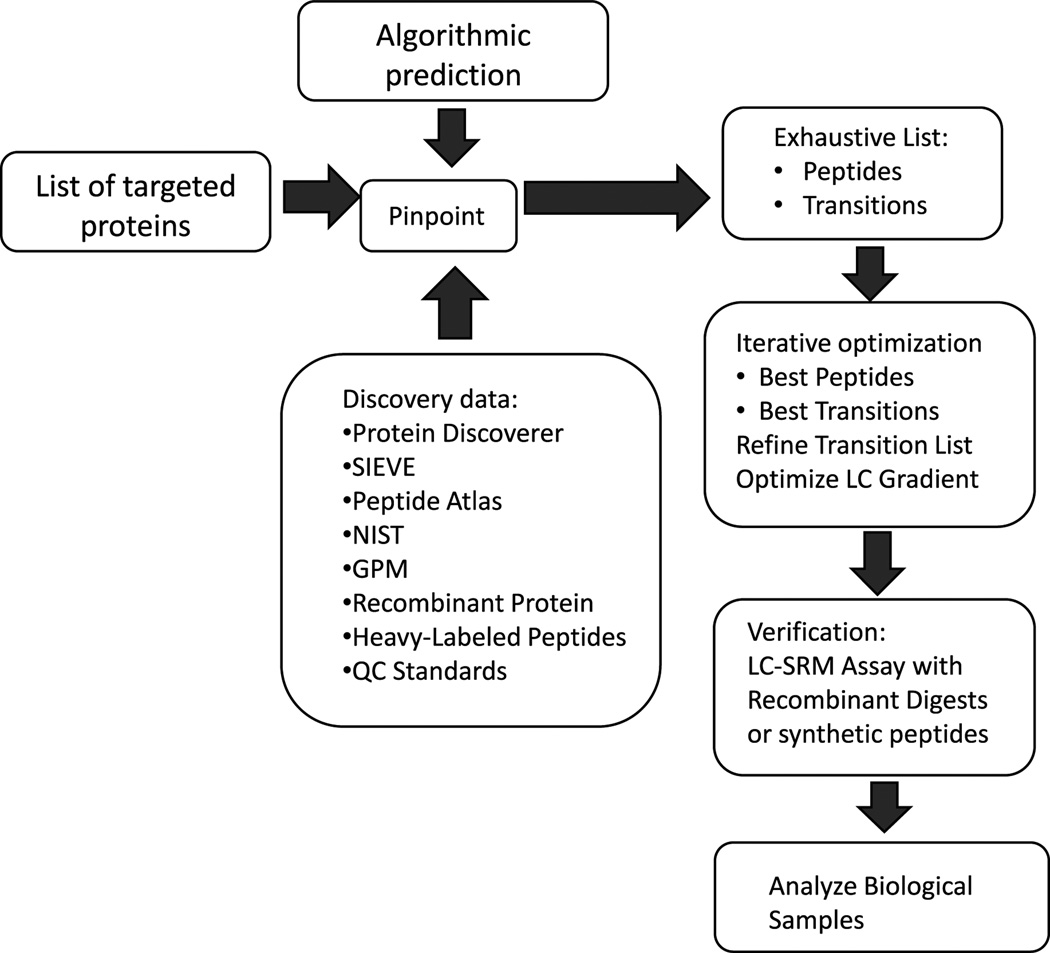
Purpose: Typically, apolipoproteins are individually measured in blood by immunoassay. In this report, we describe the development of a multiplexed selected reaction monitoring (SRM) based assay for a panel of apolipoproteins and its application to a clinical cohort of samples derived from acute stroke patients.
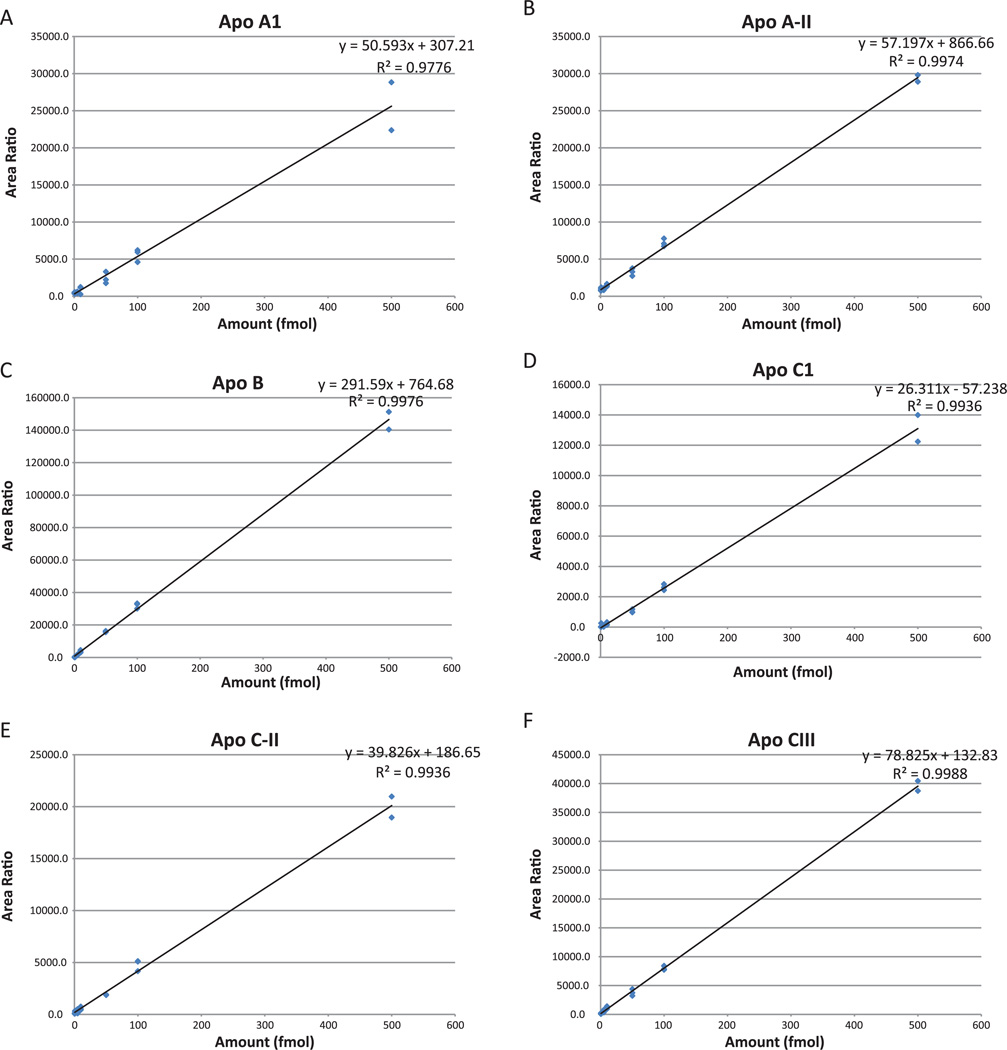
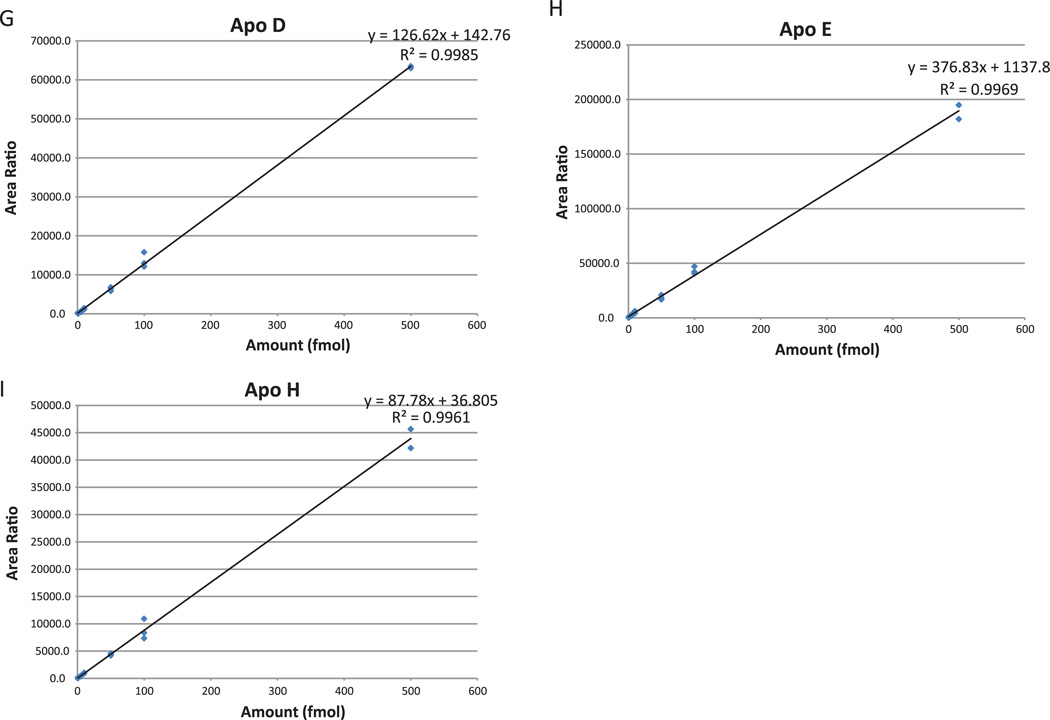
Experimental design: An SRM assay for a panel of nine apolipoproteins was developed on a triple quadrupole mass spectrometer. Quantitative data for each apolipoprotein were analyzed to determine expression ratio and receiver operating characteristic (ROC) values for ischemic versus hemorrhagic stroke.
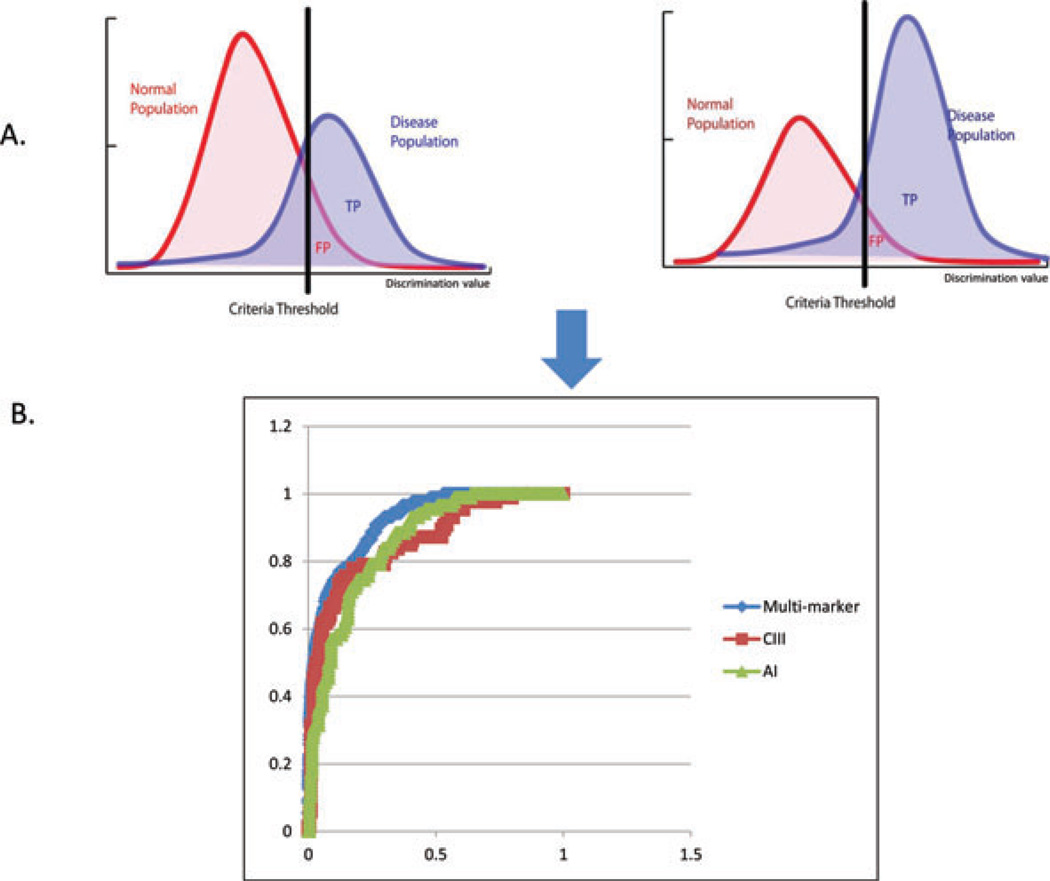
Results: The optimized SRM assay was used to interrogate a small cohort of well-characterized plasma samples obtained from patients with acute ischemic and hemorrhagic strokes. The ROC analyses demonstrated good classification power for several single apolipoproteins, most notably apoC-III and apoC-I. When a novel multi-marker ROC algorithm was applied, the ischemic versus hemorrhagic groups were best differentiated by a combination of apoC-III and apoA-I with an area under the curve (AUC) value of 0.92.
Conclusions and clinical relevance: This proof-of-concept study provides interesting and provocative data for distinguishing ischemic versus hemorrhage within first week of symptom onset. However, the observations are based on one cohort of patient samples and further confirmation will be required.
© 2012 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim.
Figures
References
-
- Elizabeth G, Nabel MD. Incidence and Prevalence: 2006 Chart Book on Cardiovascular and Lung Diseases. Bethesda, MD: National Heart, Lung, and Blood Institute; 2006.
-
- B. Kase CS, Caplan LR. Intracerebral Hemorrhage. Boston: Butterworth-Heinemann; 1996.
-
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, et al. Executive summary: heart disease and stroke statistics–2010 update: a report from the American Heart Association. Circulation. 2010;121:948–954. - PubMed
-
- Study Group. Tissue plasminogen activator for acute is-chemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N. Engl. J. Med. 1995;333:1581–1587. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
