

Systematic review of mucosal immunity induced by oral and inactivated poliovirus vaccines against virus shedding following oral poliovirus challenge
- PMID: 22532797
- PMCID: PMC3330118
- DOI: 10.1371/journal.ppat.1002599
Systematic review of mucosal immunity induced by oral and inactivated poliovirus vaccines against virus shedding following oral poliovirus challenge
Abstract
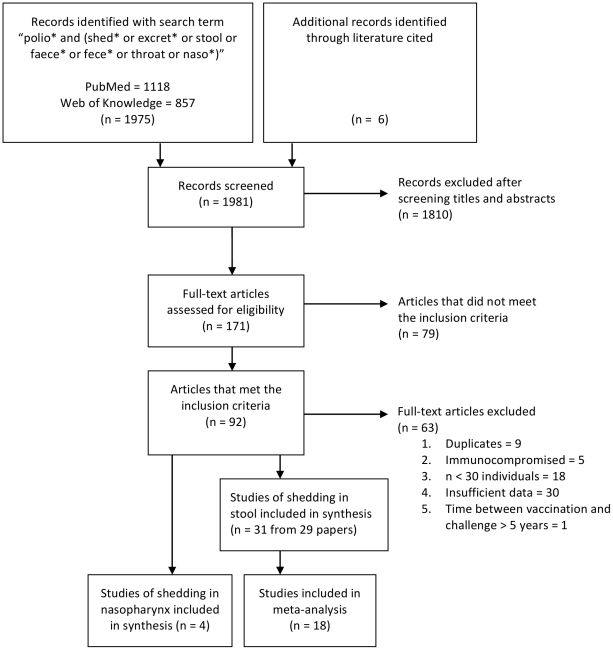
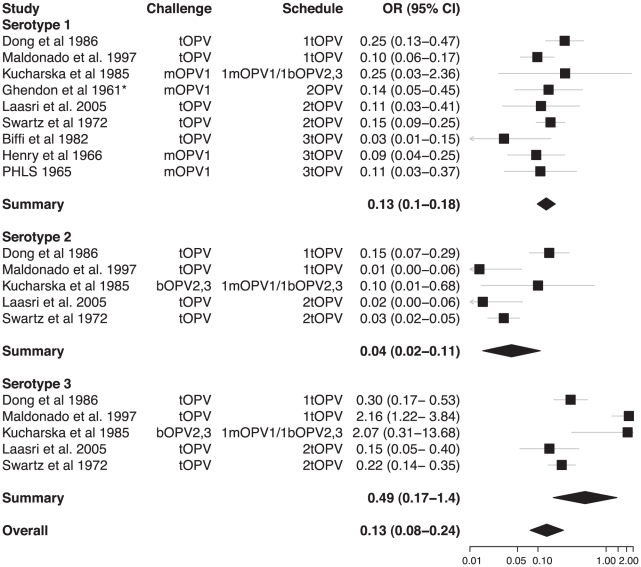
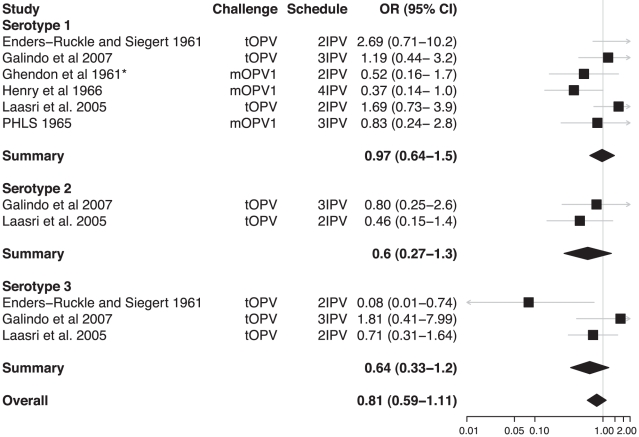
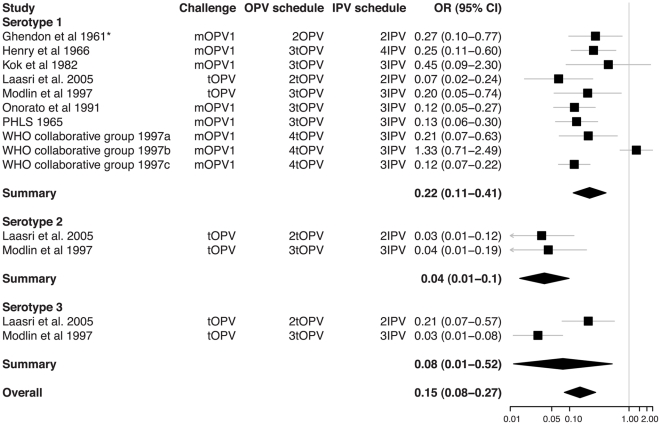
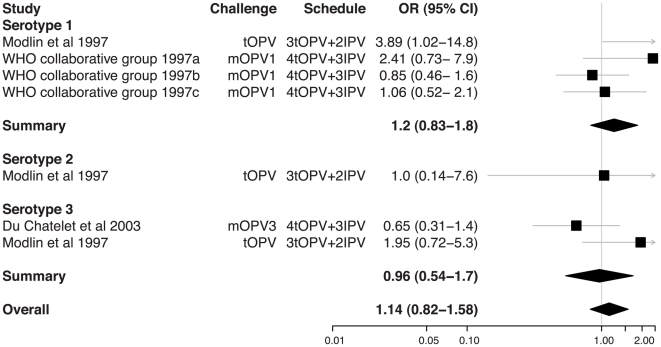
Inactivated poliovirus vaccine (IPV) may be used in mass vaccination campaigns during the final stages of polio eradication. It is also likely to be adopted by many countries following the coordinated global cessation of vaccination with oral poliovirus vaccine (OPV) after eradication. The success of IPV in the control of poliomyelitis outbreaks will depend on the degree of nasopharyngeal and intestinal mucosal immunity induced against poliovirus infection. We performed a systematic review of studies published through May 2011 that recorded the prevalence of poliovirus shedding in stool samples or nasopharyngeal secretions collected 5-30 days after a "challenge" dose of OPV. Studies were combined in a meta-analysis of the odds of shedding among children vaccinated according to IPV, OPV, and combination schedules. We identified 31 studies of shedding in stool and four in nasopharyngeal samples that met the inclusion criteria. Individuals vaccinated with OPV were protected against infection and shedding of poliovirus in stool samples collected after challenge compared with unvaccinated individuals (summary odds ratio [OR] for shedding 0.13 (95% confidence interval [CI] 0.08-0.24)). In contrast, IPV provided no protection against shedding compared with unvaccinated individuals (summary OR 0.81 [95% CI 0.59-1.11]) or when given in addition to OPV, compared with individuals given OPV alone (summary OR 1.14 [95% CI 0.82-1.58]). There were insufficient studies of nasopharyngeal shedding to draw a conclusion. IPV does not induce sufficient intestinal mucosal immunity to reduce the prevalence of fecal poliovirus shedding after challenge, although there was some evidence that it can reduce the quantity of virus shed. The impact of IPV on poliovirus transmission in countries where fecal-oral spread is common is unknown but is likely to be limited compared with OPV.
Conflict of interest statement
NCG is a member of the WHO working group on IPV that reports to the Strategic Advisory Group of Experts (SAGE) on Immunization. Otherwise, the authors have declared that no competing interests exist.
Figures
References
-
- Ogra PL, Karzon DT, Righthand F, MacGillivray M. Immunoglobulin response in serum and secretions after immunization with live and inactivated poliovaccine and natural infection. N Engl J Med. 1968;279:893–900. - PubMed
-
- Valtanen S, Roivainen M, Piirainen L, Stenvik M, Hovi T. Poliovirus-specific intestinal antibody responses coincide with decline of poliovirus excretion. J Infect Dis. 2000;182:1–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
