

Mesh reinforcement of pancreatic transection decreases incidence of pancreatic occlusion failure for left pancreatectomy: a single-blinded, randomized controlled trial
- PMID: 22534422
- PMCID: PMC3363360
- DOI: 10.1097/SLA.0b013e31825659ef
Mesh reinforcement of pancreatic transection decreases incidence of pancreatic occlusion failure for left pancreatectomy: a single-blinded, randomized controlled trial
Abstract
Introduction: Pancreatic leak or fistula is the most frequent complication after left pancreatectomy. We performed a single-blinded, parallel-group, randomized controlled trial comparing stapled left pancreatectomy with stapled left pancreatectomy using mesh reinforcement of the staple line with either Seamguard or Peristrips Dry.
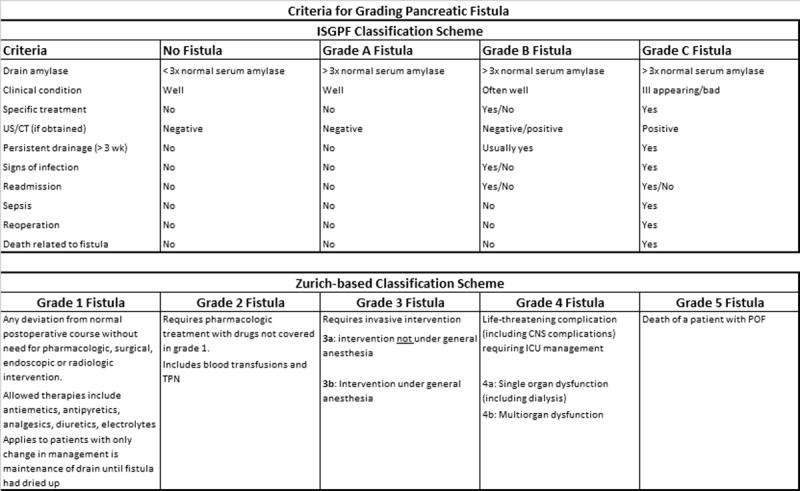
Methods: All patients undergoing left pancreatectomy at a large tertiary hospital were eligible for participation. Patients were randomized to either mesh reinforcement or no-mesh reinforcement intraoperatively after being determined a candidate for resection. Patients were blinded to the result of their randomization for 6 weeks. Primary outcome measure was clinically significant leak as defined by the ISGPF (International Study Group on Pancreatic Fistula) pancreatic leak grading system.
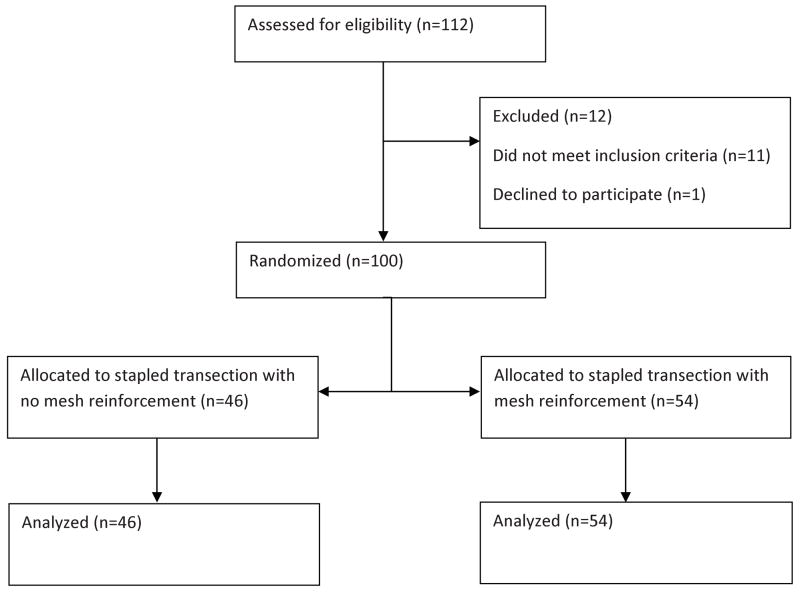
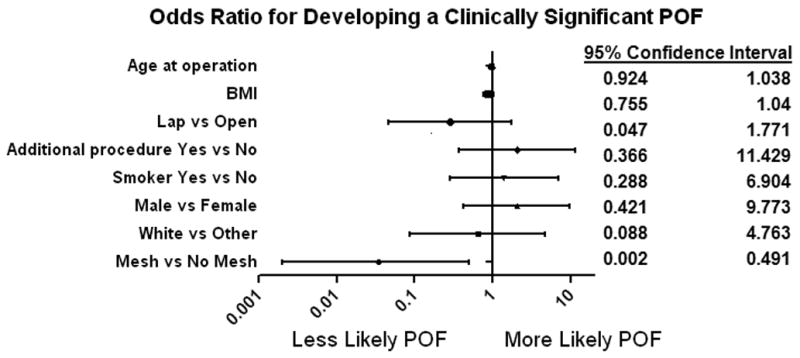
Results: One hundred patients were randomized to either mesh (54) or no-mesh (46) reinforcement of their pancreatic transection. There was 1 death in each group. ISGPF grade B and C leaks were seen in 1.9% (1/53) of patients undergoing resection with mesh reinforcement and 20% (11/45) of patients without mesh reinforcement (P = .0007).
Conclusions: Mesh reinforcement of pancreatic transection line significantly reduces the incidence of significant pancreatic fistula in patients undergoing left pancreatectomy.
Trial registration: Clinicaltrials.gov: NCT01359410.
Figures
Comment in
-
[Mesh-enforced stapling for left pancreatectomy. A solution to the problem of pancreatic fistula?].Chirurg. 2012 Sep;83(9):821. doi: 10.1007/s00104-012-2359-x. Chirurg. 2012. PMID: 22911270 German. No abstract available.
References
-
- Knaebel HP, Diener MK, Wenter MN, et al. Systematic review and meta-analysis of technique for closure of the pancreatic remnant after distal pancreatectomy. Br J Surg. 2005;92:539–46. - PubMed
-
- Bilimoria MM, Cormier JN, Mun Y, Lee JE, Evans DB, Pisters PWT. Pancreatic leak after left pancreatectomy is reduced following main pancreatic duct ligation. Br J Surg. 2003;90:190–196. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
