

Risk of contrast induced nephropathy in the critically ill: a prospective, case matched study
- PMID: 22534554
- PMCID: PMC3681396
- DOI: 10.1186/cc11317
Risk of contrast induced nephropathy in the critically ill: a prospective, case matched study
Abstract
Introduction: Computerized tomography is frequently employed in the critically ill, often using intravenous radiocontrast material. Many of these patients have clinical features that are considered risk factors for contrast induced nephropathy, but are simultaneously at risk for renal injury from other factors related to their acute illnesses. The attributable risk for renal dysfunction from radiocontrast exposure has not been well quantified in this population.
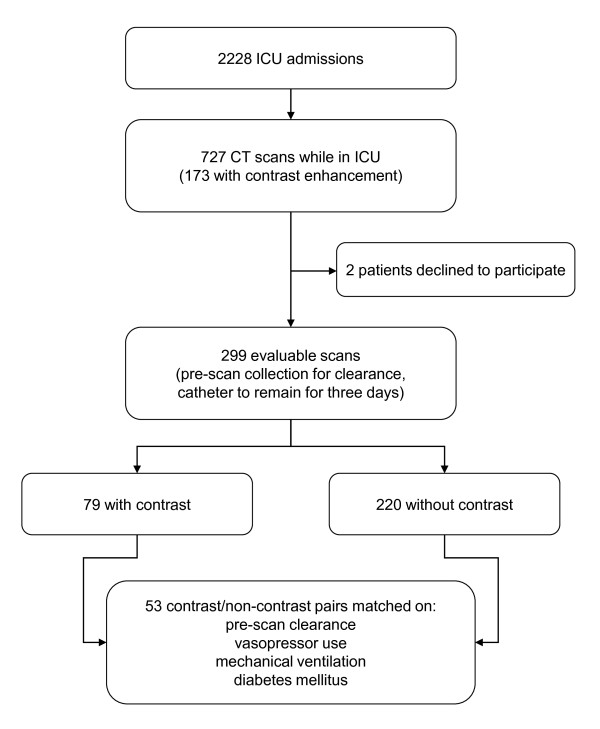
Methods: A prospective matched cohort study was conducted of patients scanned with or without radiocontrast enhancement while receiving intensive care in a Veterans Affairs Medical Center. Patients were matched for pre-scan measured creatinine clearance, diabetes, mechanical ventilation, and vasopressor use. Measured clearance was followed for three days after scanning. Evolution of nephropathy, as determined by change in measured clearance, was compared within matched pairs.
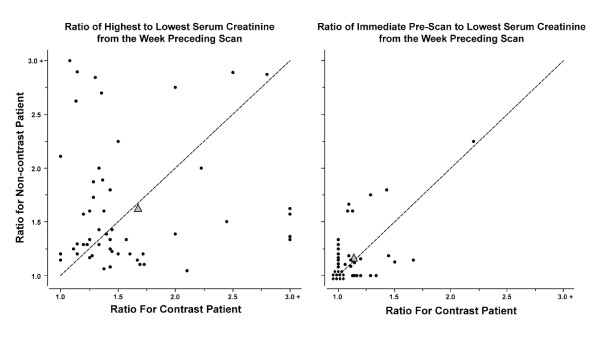
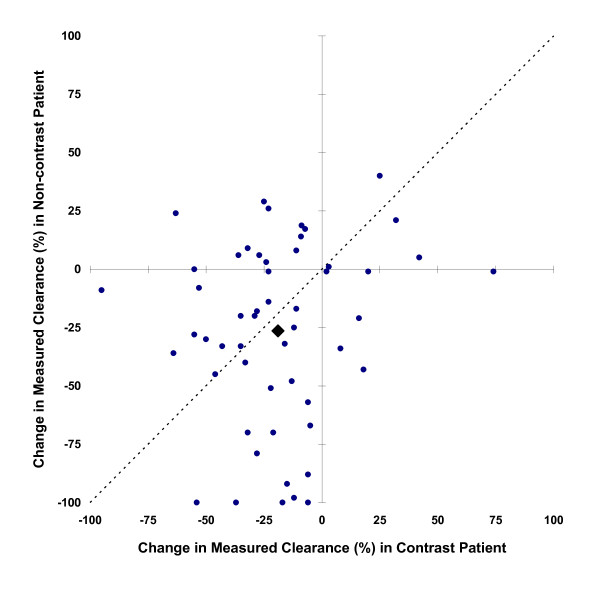
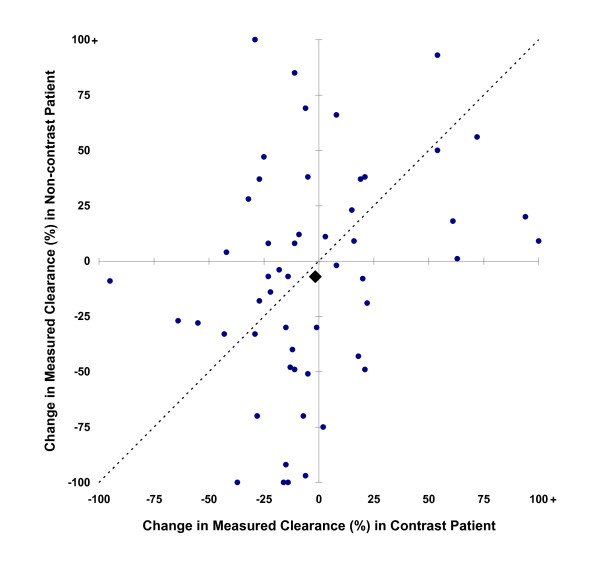
Results: Fifty-three pairs of patients satisfied matching criteria. Unmatched characteristics were similar among the pairs, including serum creatinine variability during the week preceding scanning (67 ± 85% among contrast recipients, 63 ± 62% among others) and clinical risk factors for renal failure. In 29 pairs, pre-scan measured clearances were less than 60 mL/minute/1.73 m2. Following scanning, measured clearance declined by at least 33% in 14 contrast and 19 non-contrast patients (95% confidence interval for contrast associated difference in nephropathy rates -27% to 9%), while a 50% reduction in clearance persisted three days after scanning in three contrast and nine non-contrast patients (95% confidence interval for difference in rates -25% to 2%).
Conclusions: Among established intensive care unit patients declines in glomerular filtration following contrast-enhanced scanning are common, but these changes are far more likely to be attributable to factors other than the contrast exposure itself. The upper bound for the incidence of contrast induced renal injury lasting even three days was 2% in the population studied.
Figures
Comment in
-
Contrast-induced nephropathy: attributable incidence and potential harm.Crit Care. 2012 May 23;16(3):127. doi: 10.1186/cc11327. Crit Care. 2012. PMID: 22621609 Free PMC article.
References
-
- Tumlin J, Stacul F, Adam A, Becker CR, Davidson C, Lameire N, McCullough PA. Pathophysiology of contrast-induced nephropathy. Am J Cardiol. 2006;16:14K–20K. - PubMed
-
- Briguori C, Airoldi F, D'Andrea D, Bonizzoni E, Morici N, Focaccio A, Michev I, Montorfano M, Carlino M, Cosgrave J, Ricciardelli B, Colombo A. Renal Insufficiency Following Contrast Media Administration Trial (REMEDIAL): a randomized comparison of 3 preventive strategies. Circulation. 2007;16:1211–1217. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
