

Margin size is an independent predictor of local tumor progression after ablation of colon cancer liver metastases
- PMID: 22535243
- PMCID: PMC4122121
- DOI: 10.1007/s00270-012-0377-1
Margin size is an independent predictor of local tumor progression after ablation of colon cancer liver metastases
Abstract
Purpose: This study was designed to evaluate the relationship between the minimal margin size and local tumor progression (LTP) following CT-guided radiofrequency ablation (RFA) of colorectal cancer liver metastases (CLM).
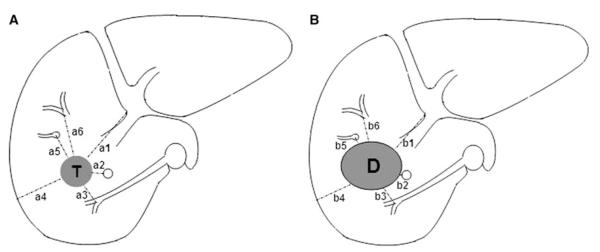
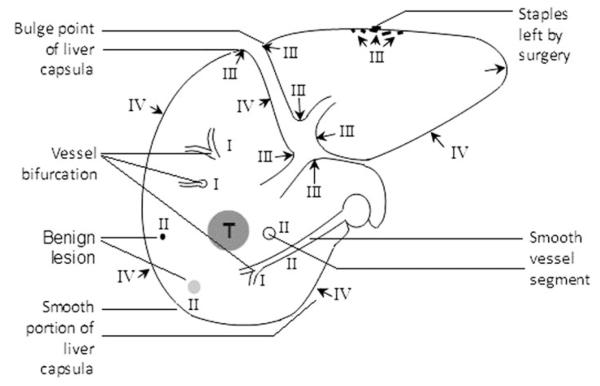
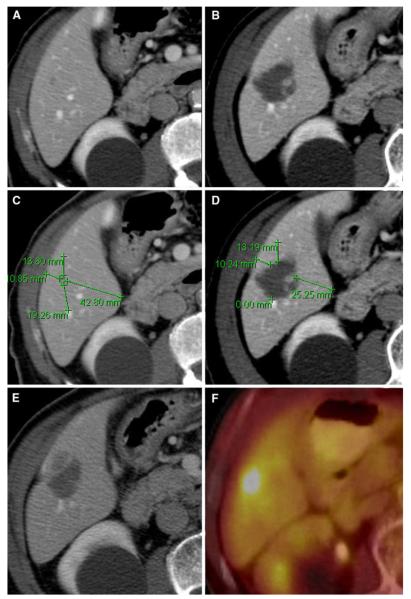
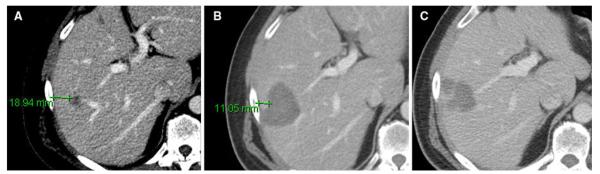
Methods: An institutional review board-approved, HIPPA-compliant review identified 73 patients with 94 previously untreated CLM that underwent RFA between March 2003 and May 2010, resulting in an ablation zone completely covering the tumor 4-8 weeks after RFA dynamic CT. Comparing the pre- with the post-RFA CT, the minimal margin size was categorized to 0, 1-5, 6-10, and 11-15 mm. Follow-up included CT every 2-4 months. Kaplan-Meier methodology and Cox regression analysis were used to evaluate the effect of the minimal margin size, tumor location, size, and proximity to a vessel on LTP.
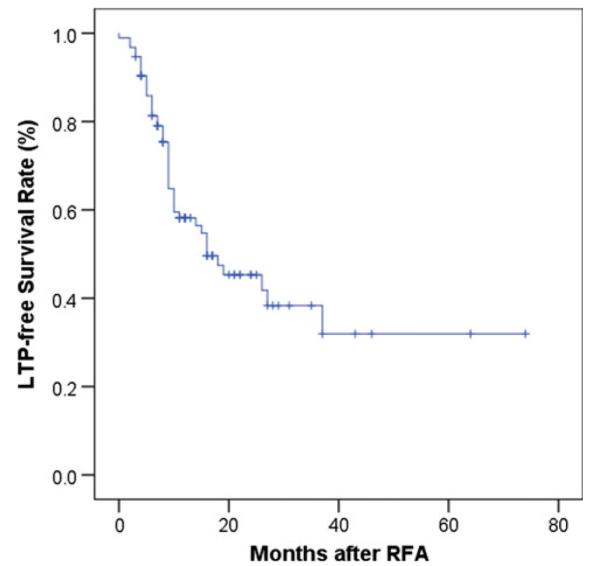
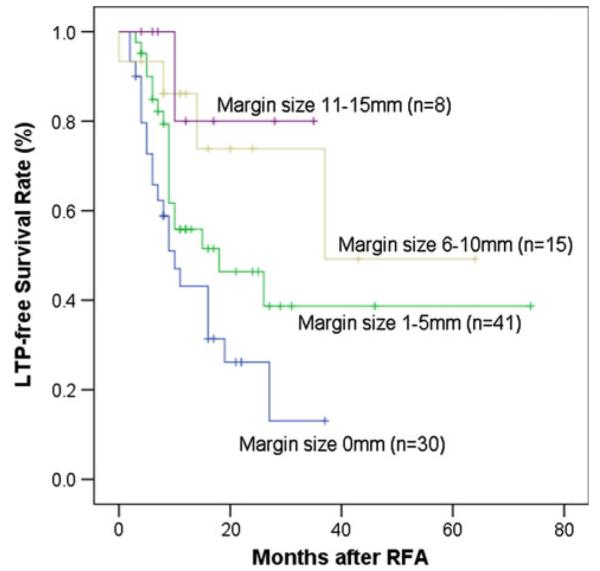
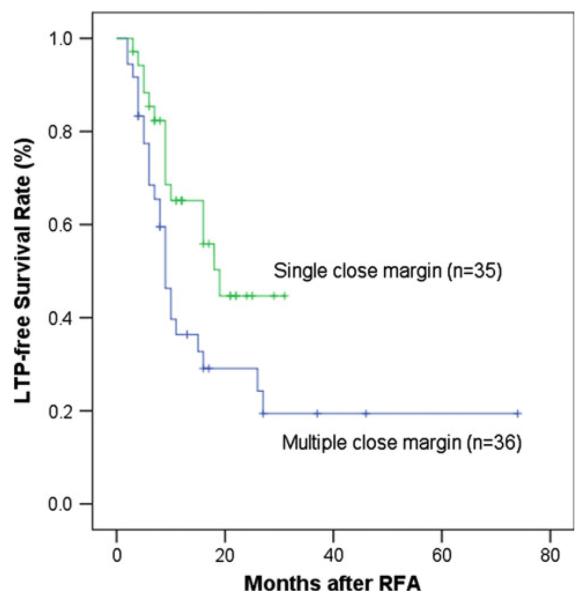
Results: Forty-five of 94 (47.9 %) CLM progressed locally. Median LTP-free survival (LPFS) was 16 months. Two-year LPFS rates for ablated CLM with minimal margin of 0, 1-5 mm, 6-10 mm, 11-15 mm were 26, 46, 74, and 80 % (p < 0.011). Minimal margin (p = 0.002) and tumor size (p = 0.028) were independent risk factors for LTP. The risk for LTP decreased by 46 % for each 5-mm increase in minimal margin size, whereas each additional 5-mm increase in tumor size increased the risk of LTP by 22 %.
Conclusions: An ablation zone with a minimal margin uniformly larger than 5 mm 4-8 weeks postablation CT is associated with the best local tumor control.
Figures

References
-
- Berber E, Siperstein A. Local recurrence after laparoscopic radiofrequency ablation of liver tumors: an analysis of 1032 tumors. Ann Surg Oncol. 2008;15(10):2757–2764. - PubMed
-
- Mulier S, Ruers T, Jamart J, Michel L, Marchal G, Ni Y. Radiofrequency ablation versus resection for resectable colorectal liver metastases: time for a randomized trial? An update. Dig Surg. 2008;25(6):445–460. - PubMed
-
- Leen E, Horgan PG. Radiofrequency ablation of colorectal liver metastases. Surg Oncol. 2007;16(1):47–51. - PubMed
-
- Ayav A, Germain A, Marchal F, et al. Radiofrequency ablation of unresectable liver tumors: factors associated with incomplete ablation or local recurrence. Am J Surg. 2010;200(4):435–439. - PubMed
-
- Sofocleous C, Nascimento R, Petrovic L, et al. Histopathology of tissue extracted on the probe after radiofrequency ablation of liver malignancy can predict local progression: initial results. Radiology. 2008;249(1(Oct)):364–374. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
