

Metabolic slowing with massive weight loss despite preservation of fat-free mass
- PMID: 22535969
- PMCID: PMC3387402
- DOI: 10.1210/jc.2012-1444
Metabolic slowing with massive weight loss despite preservation of fat-free mass
Erratum in
-
Corrigenda.J Clin Endocrinol Metab. 2016 May;101(5):2266. doi: 10.1210/jc.2016-1651. J Clin Endocrinol Metab. 2016. PMID: 27163466 Free PMC article. No abstract available.
Abstract
Context: An important goal during weight loss is to maximize fat loss while preserving metabolically active fat-free mass (FFM). Massive weight loss typically results in substantial loss of FFM potentially slowing metabolic rate.
Objective: Our objective was to determine whether a weight loss program consisting of diet restriction and vigorous exercise helped to preserve FFM and maintain resting metabolic rate (RMR).
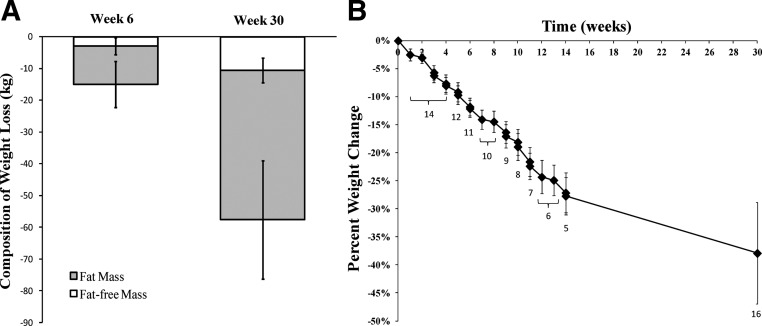
Participants and intervention: We measured body composition by dual-energy x-ray absorptiometry, RMR by indirect calorimetry, and total energy expenditure by doubly labeled water at baseline (n = 16), wk 6 (n = 11), and wk 30 (n = 16).
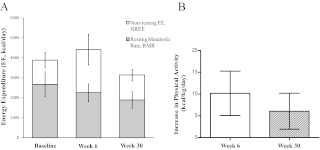
Results: At baseline, participants were severely obese (× ± SD; body mass index 49.4 ± 9.4 kg/m(2)) with 49 ± 5% body fat. At wk 30, more than one third of initial body weight was lost (-38 ± 9%) and consisted of 17 ± 8% from FFM and 83 ± 8% from fat. RMR declined out of proportion to the decrease in body mass, demonstrating a substantial metabolic adaptation (-244 ± 231 and -504 ± 171 kcal/d at wk 6 and 30, respectively, P < 0.01). Energy expenditure attributed to physical activity increased by 10.2 ± 5.1 kcal/kg.d at wk 6 and 6.0 ± 4.1 kcal/kg.d at wk 30 (P < 0.001 vs. zero).
Conclusions: Despite relative preservation of FFM, exercise did not prevent dramatic slowing of resting metabolism out of proportion to weight loss. This metabolic adaptation may persist during weight maintenance and predispose to weight regain unless high levels of physical activity or caloric restriction are maintained.
Figures
References
-
- Sturm R. 2003. Increases in clinically severe obesity in the United States, 1986–2000. Arch Intern Med 163:2146–2148 - PubMed
-
- Wang YC, McPherson K, Marsh T, Gortmaker SL, Brown M. 2011. Health and economic burden of the projected obesity trends in the USA and the UK. Lancet 378:815–825 - PubMed
-
- Buchwald H, Oien DM. 2009. Metabolic/bariatric surgery Worldwide 2008. Obes Surg 19:1605–1611 - PubMed
-
- Pontiroli AE, Morabito A. 2011. Long-term prevention of mortality in morbid obesity through bariatric surgery. a systematic review and meta-analysis of trials performed with gastric banding and gastric bypass. Ann Surg 253:484–487 - PubMed
-
- Chaston TB, Dixon JB, O'Brien PE. 2007. Changes in fat-free mass during significant weight loss: a systematic review. Int J Obes (Lond) 31:743–750 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
