

Microcystic macular oedema in multiple sclerosis is associated with disease severity
- PMID: 22539259
- PMCID: PMC3359753
- DOI: 10.1093/brain/aws098
Microcystic macular oedema in multiple sclerosis is associated with disease severity
Abstract
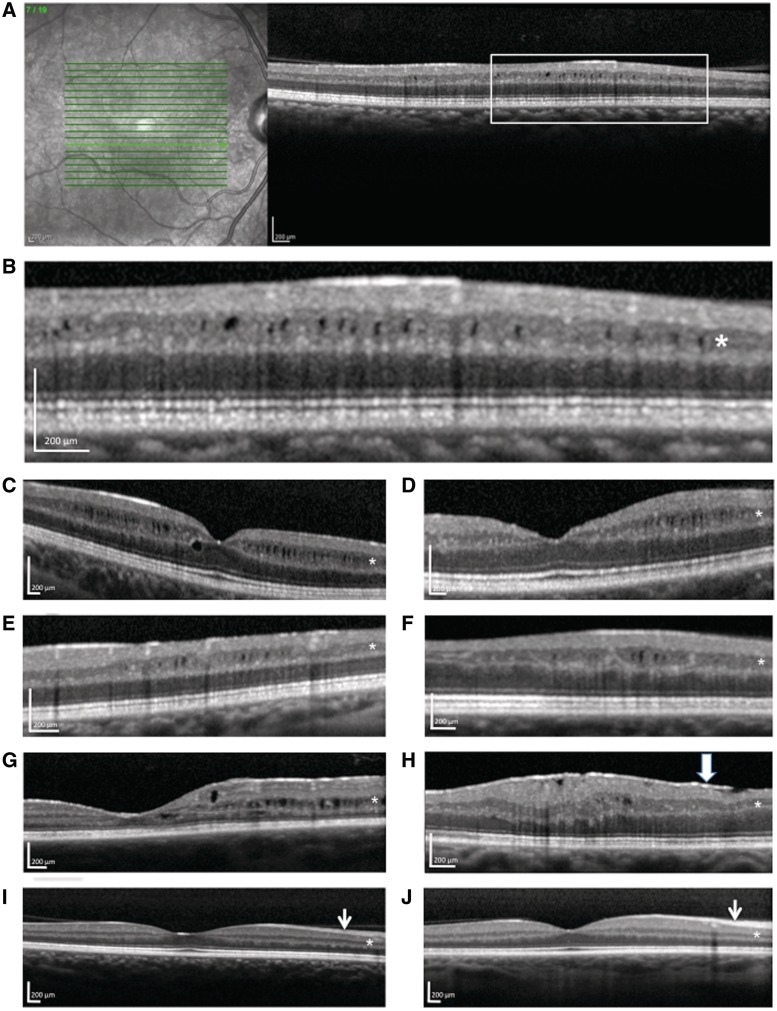
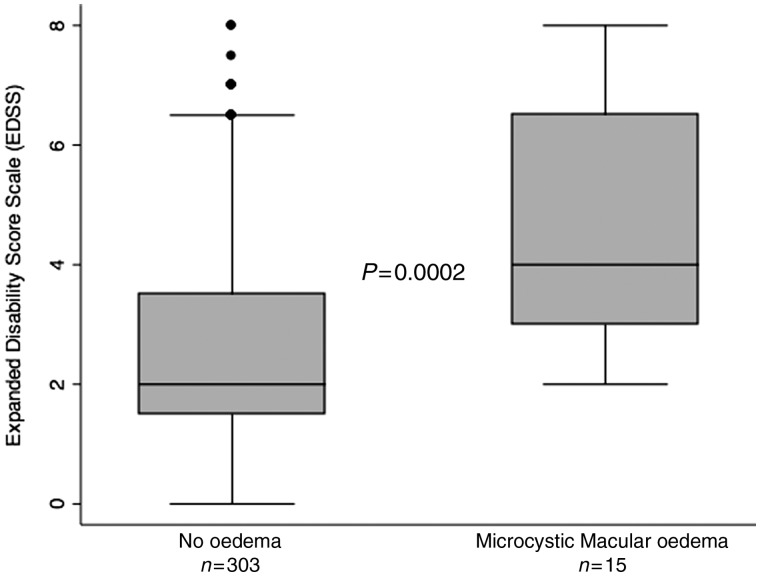
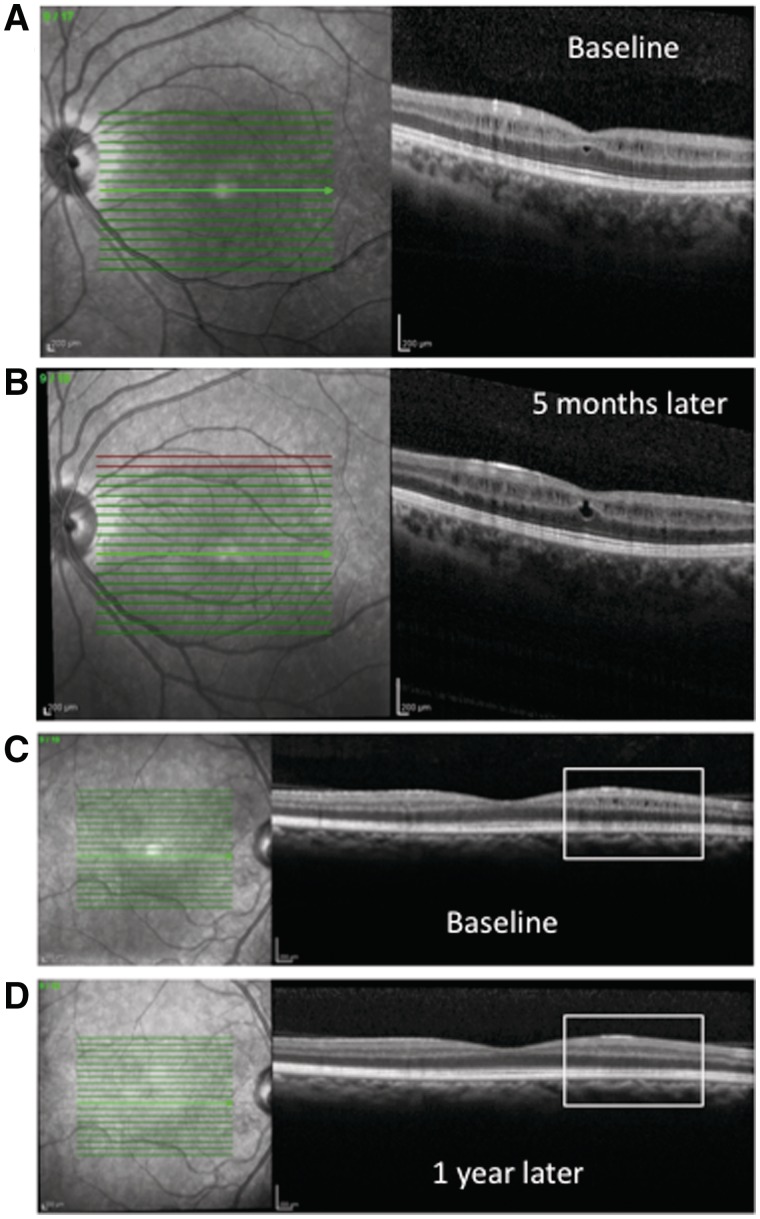
Macular oedema typically results from blood-retinal barrier disruption. It has recently been reported that patients with multiple sclerosis treated with FTY-720 (fingolimod) may exhibit macular oedema. Multiple sclerosis is not otherwise thought to be associated with macular oedema except in the context of comorbid clinical uveitis. Despite a lack of myelin, the retina is a site of inflammation and microglial activation in multiple sclerosis and demonstrates significant neuronal and axonal loss. We unexpectedly observed microcystic macular oedema using spectral domain optical coherence tomography in patients with multiple sclerosis who did not have another reason for macular oedema. We therefore evaluated spectral domain optical coherence tomography images in consecutive patients with multiple sclerosis for microcystic macular oedema and examined correlations between macular oedema and visual and ambulatory disability in a cross-sectional analysis. Participants were excluded if there was a comorbidity that could account for the presence of macular oedema, such as uveitis, diabetes or other retinal disease. A microcystic pattern of macular oedema was observed on optical coherence tomography in 15 of 318 (4.7%) patients with multiple sclerosis. No macular oedema was identified in 52 healthy controls assessed over the same period. The microcystic oedema predominantly involved the inner nuclear layer of the retina and tended to occur in small, discrete patches. Patients with multiple sclerosis with microcystic macular oedema had significantly worse disability [median Expanded Disability Score Scale 4 (interquartile range 3-6)] than patients without macular oedema [median Expanded Disability Score Scale 2 (interquartile range 1.5-3.5)], P = 0.0002. Patients with multiple sclerosis with microcystic macular oedema also had higher Multiple Sclerosis Severity Scores, a measure of disease progression, than those without oedema [median of 6.47 (interquartile range 4.96-7.98) versus 3.65 (interquartile range 1.92-5.87), P = 0.0009]. Microcystic macular oedema occurred more commonly in eyes with prior optic neuritis than eyes without prior optic neuritis (50 versus 27%) and was associated with lower visual acuity (median logMAR acuity of 0.17 versus -0.1) and a thinner retinal nerve fibre layer. The presence of microcystic macular oedema in multiple sclerosis suggests that there may be breakdown of the blood-retinal barrier and tight junction integrity in a part of the nervous system that lacks myelin. Microcystic macular oedema may also contribute to visual dysfunction beyond that explained by nerve fibre layer loss. Microcystic changes need to be assessed, and potentially adjusted for, in clinical trials that evaluate macular volume as a marker of retinal ganglion cell survival. These findings also have implications for clinical monitoring in patients with multiple sclerosis on sphingosine 1-phosphate receptor modulating agents.
Figures
Comment in
-
Microcystic macular degeneration from optic neuropathy.Brain. 2012 Dec;135(Pt 12):e225. doi: 10.1093/brain/aws215. Epub 2012 Sep 7. Brain. 2012. PMID: 22960546 No abstract available.
-
Microcystic macular oedema confirmed, but not specific for multiple sclerosis.Brain. 2012 Dec;135(Pt 12):e226; author reply e227. doi: 10.1093/brain/aws216. Epub 2012 Oct 17. Brain. 2012. PMID: 23078994 Free PMC article. No abstract available.
-
Microcystic macular degeneration from optic neuropathy: not inflammatory, not trans-synaptic degeneration.Brain. 2013 Jul;136(Pt 7):e239. doi: 10.1093/brain/awt014. Epub 2013 Feb 8. Brain. 2013. PMID: 23396580 No abstract available.
-
Reply: Microcystic macular degeneration from optic neuropathy: not inflammatory, not trans-synaptic degeneration.Brain. 2013 Jul;136(Pt 7):e240. doi: 10.1093/brain/awt018. Epub 2013 Feb 8. Brain. 2013. PMID: 23650224 Free PMC article. No abstract available.
-
Reply: Microcysts in the inner nuclear layer from optic atrophy are caused by retrograde trans-synaptic degeneration combined with vitreous traction on the retinal surface.Brain. 2013 Nov;136(Pt 11):e261. doi: 10.1093/brain/awt155. Epub 2013 Jul 19. Brain. 2013. PMID: 23872367 No abstract available.
-
Microcysts in the inner nuclear layer from optic atrophy are caused by retrograde trans-synaptic degeneration combined with vitreous traction on the retinal surface.Brain. 2013 Nov;136(Pt 11):e260. doi: 10.1093/brain/awt154. Epub 2013 Jul 19. Brain. 2013. PMID: 23872368 Free PMC article. No abstract available.
References
-
- Burkholder BM, Osborne B, Loguidice MJ, Bisker E, Frohman TC, Conger A, et al. Macular volume determined by optical coherence tomography as a measure of neuronal loss in multiple sclerosis. Arch Neurol. 2009;66:1366–72. - PubMed
-
- Cohen JA, Barkhof F, Comi G, Hartung HP, Khatri BO, Montalban X, et al. Oral fingolimod or intramuscular interferon for relapsing multiple sclerosis. N Engl J Med. 2010;362:402–15. - PubMed
-
- Costello F, Coupland S, Hodge W, Lorello GR, Koroluk J, Pan YI, et al. Quantifying axonal loss after optic neuritis with optical coherence tomography. Ann Neurol. 2006;59:963–9. - PubMed
-
- Costello F, Hodge W, Pan YI, Freedman M, DeMeulemeester C. Differences in retinal nerve fiber layer atrophy between multiple sclerosis subtypes. J Neurol Sci. 2009;281:74–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
