

Renal function at hospital admission and mortality due to acute kidney injury after myocardial infarction
- PMID: 22539974
- PMCID: PMC3335121
- DOI: 10.1371/journal.pone.0035496
Renal function at hospital admission and mortality due to acute kidney injury after myocardial infarction
Abstract
Background: The role of an impaired estimated glomerular filtration rate (eGFR) at hospital admission in the outcome of acute kidney injury (AKI) after acute myocardial infarction (AMI) has been underreported. The aim of this study was to assess the influence of an admission eGFR<60 mL/min/1.73 m(2) on the incidence and early and late mortality of AMI-associated AKI.
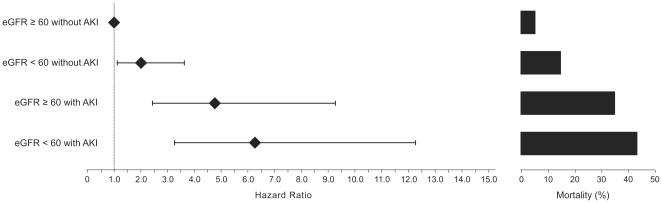
Methods: A prospective study of 828 AMI patients was performed. AKI was defined as a serum creatinine increase of ≥ 50% from the time of admission (RIFLE criteria) in the first 7 days of hospitalization. Patients were divided into subgroups according to their eGFR upon hospital admission (MDRD formula, mL/min/1.73 m(2)) and the development of AKI: eGFR ≥ 60 without AKI, eGFR<60 without AKI, eGFR ≥ 60 with AKI and eGFR<60 with AKI.
Results: Overall, 14.6% of the patients in this study developed AKI. The admission eGFR had no impact on the incidence of AKI. However, the admission eGFR was associated with the outcome of AMI-associated AKI. The adjusted hazard ratios (AHR, Cox multivariate analysis) for 30-day mortality were 2.00 (95% CI 1.11-3.61) for eGFR<60 without AKI, 4.76 (95% CI 2.45-9.26) for eGFR ≥ 60 with AKI and 6.27 (95% CI 3.20-12.29) for eGFR<60 with AKI. Only an admission eGFR of <60 with AKI was significantly associated with a 30-day to 1-year mortality hazard (AHR 3.05, 95% CI 1.50-6.19).
Conclusions: AKI development was associated with an increased early mortality hazard in AMI patients with either preserved or impaired admission eGFR. Only the association of impaired admission eGFR and AKI was associated with an increased hazard for late mortality among these patients.
Conflict of interest statement
Figures



References
-
- Ali T, Khan I, Simpson W, Prescott G, Townend J, et al. Incidence and outcomes in acute kidney injury: a comprehensive population-based study. J Am Soc Nephrol. 2007;18:1292–1298. - PubMed
-
- Collins AJ, Foley RN, Herzog C, Chavers B, Gilbertson D, et al. United States Renal Data System 2008 Annual Data Report. Am J Kidney Dis. 2009;57:S1–374. - PubMed
-
- Goldberg A, Hammerman H, Petcherski S, Zdorovyak A, Yalonetsky S, et al. Inhospital and 1-year mortality of patients who develop worsening renal function following acute ST-elevation myocardial infarction. Am Heart J. 2005;150:330–337. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
