

Impact of HbA1c Criterion on the Detection of Subjects with Increased Risk for Diabetes among Health Check-Up Recipients in Korea
- PMID: 22540052
- PMCID: PMC3335897
- DOI: 10.4093/dmj.2012.36.2.151
Impact of HbA1c Criterion on the Detection of Subjects with Increased Risk for Diabetes among Health Check-Up Recipients in Korea
Abstract
Background: We performed the study to examine the impact of hemoglobin A1c (HbA1c) criterion on the screening of increased risk for diabetes among health check-up subjects in Korea.
Methods: We retrospectively analyzed clinical and laboratory data of 37,754 Korean adults (age, 20 to 89 years; 41% women) which were measured during regular health check-ups. After excluding subjects with previously diagnosed diabetes mellitus (n=1,812) and with overt anemia (n=318), 35,624 subjects (21,201 men and 14,423 women) were included in the analysis.
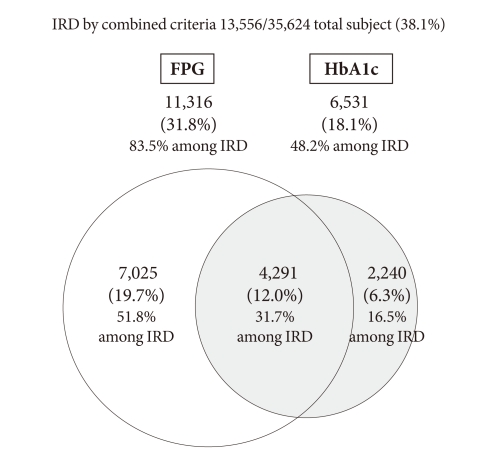
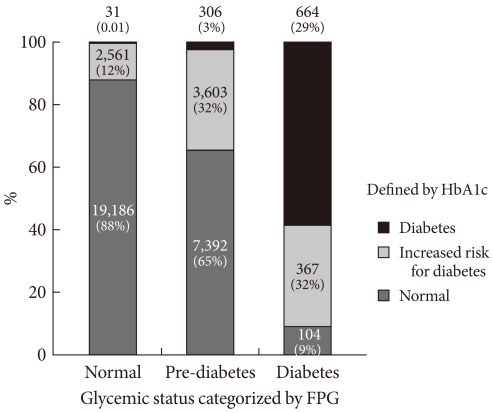
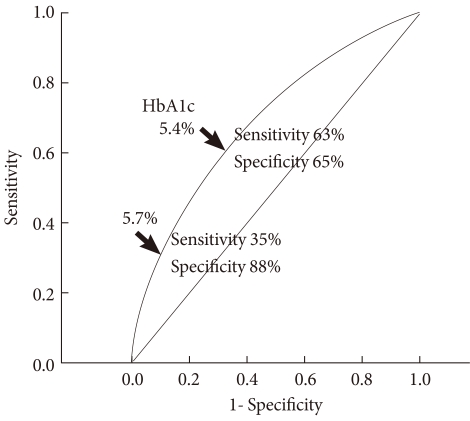
Results: Among the 35,624 subjects, 11,316 (31.8%) subjects were categorized as increased risk for diabetes (IRD) by fasting plasma glucose (FPG) criteria, 6,531 (18.1%) subjects by HbA1c criteria, and 13,556 (38.1%) subjects by combined criteria. Therefore, although HbA1c criteria alone identifies 42% [(11,316-6,531)/11,316] fewer subjects with IRD than does FPG criteria, about 20% [(13,556-11,316)/11,316] more subjects could be detected by including new HbA1c criteria in addition to FPG criteria. Among the 13,556 subjects with IRD, 7,025 (51.8%) met FPG criteria only, 2,240 (16.5%) met HbA1c criteria only, and 4,291 (31.7%) met both criteria. Among subjects with impaired fasting glucose, 65% were normal, 32% were IRD, and 3% were diabetes by HbA1c criterion. In receiver operating characteristic curve analysis, cutoff point of HbA1c with optimal sensitivity and specificity for identifying IRD was 5.4%.
Conclusion: Although HbA1c criteria alone identifies fewer subjects with IRD than does FPG criteria, about 20% more could be detected by addition of HbA1c criteria. Further studies are needed to define optimal cutoff point of HbA1c and to establish screening and management guidelines for IRD.
Keywords: Fasting plasma glucose; Hemoglobin A, glycosylated; Prediabetic state; Prevalence.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Herman WH, Ma Y, Uwaifo G, Haffner S, Kahn SE, Horton ES, Lachin JM, Montez MG, Brenneman T, Barrett-Connor E Diabetes Prevention Program Research Group. Differences in A1C by race and ethnicity among patients with impaired glucose tolerance in the Diabetes Prevention Program. Diabetes Care. 2007;30:2453–2457. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
