

Cerebrospinal fluid levels of high-mobility group box 1 and cytochrome C predict outcome after pediatric traumatic brain injury
- PMID: 22540160
- PMCID: PMC3408241
- DOI: 10.1089/neu.2011.2171
Cerebrospinal fluid levels of high-mobility group box 1 and cytochrome C predict outcome after pediatric traumatic brain injury
Abstract
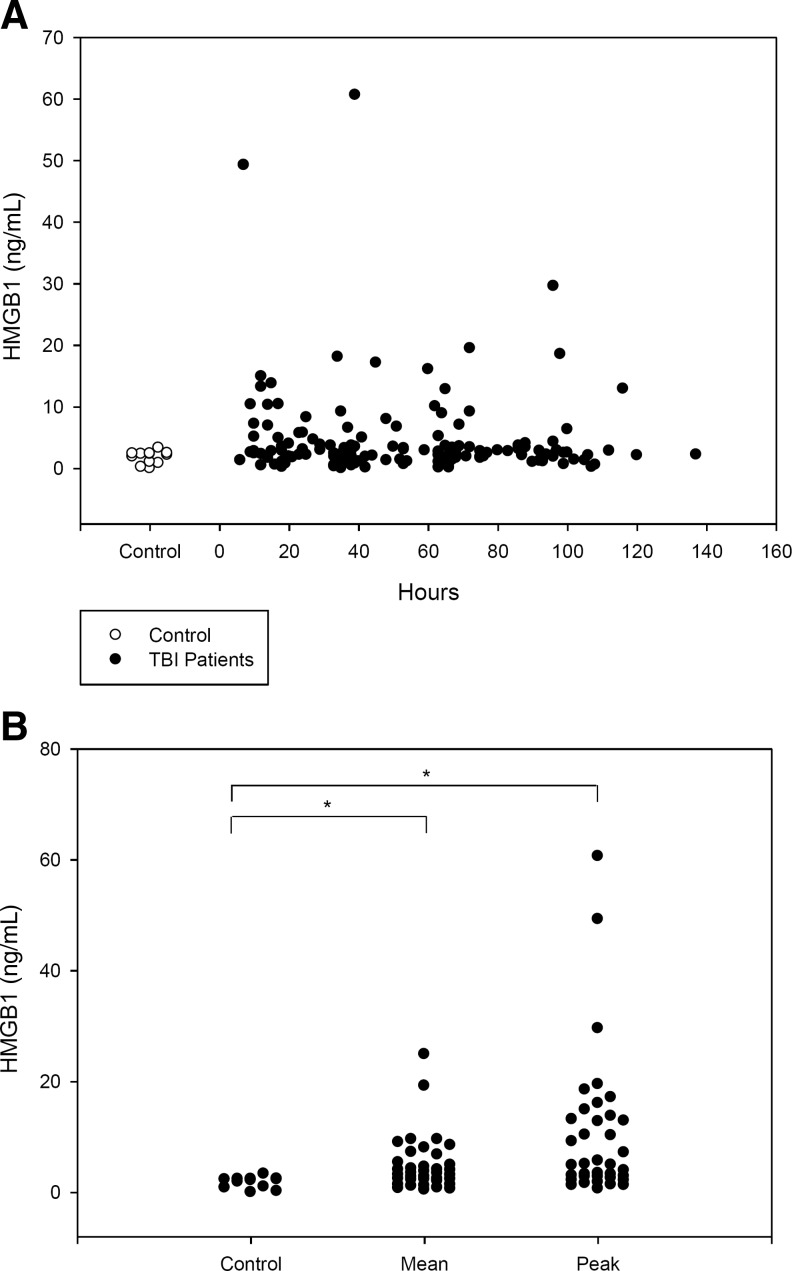
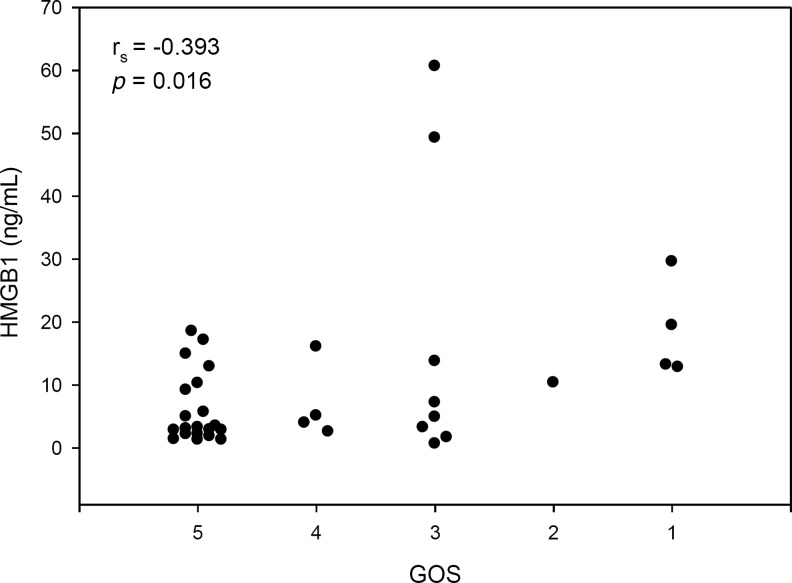
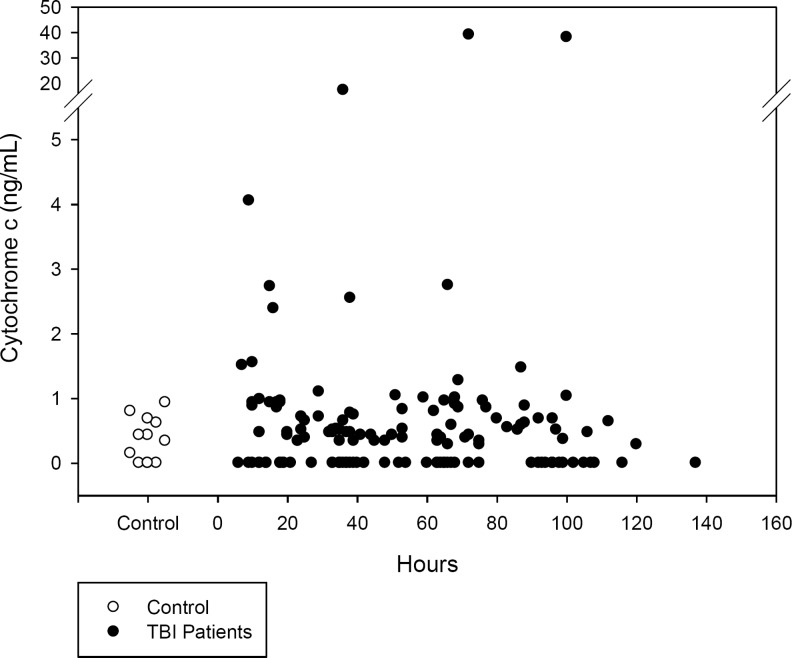
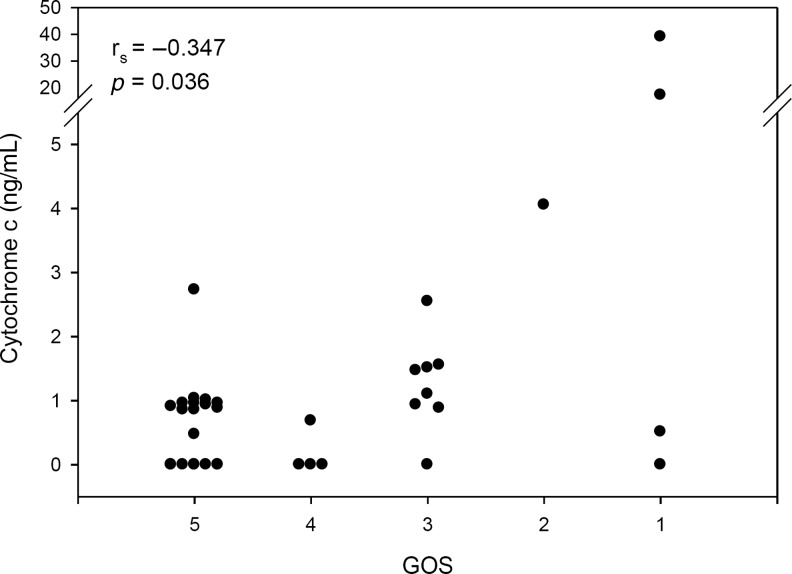
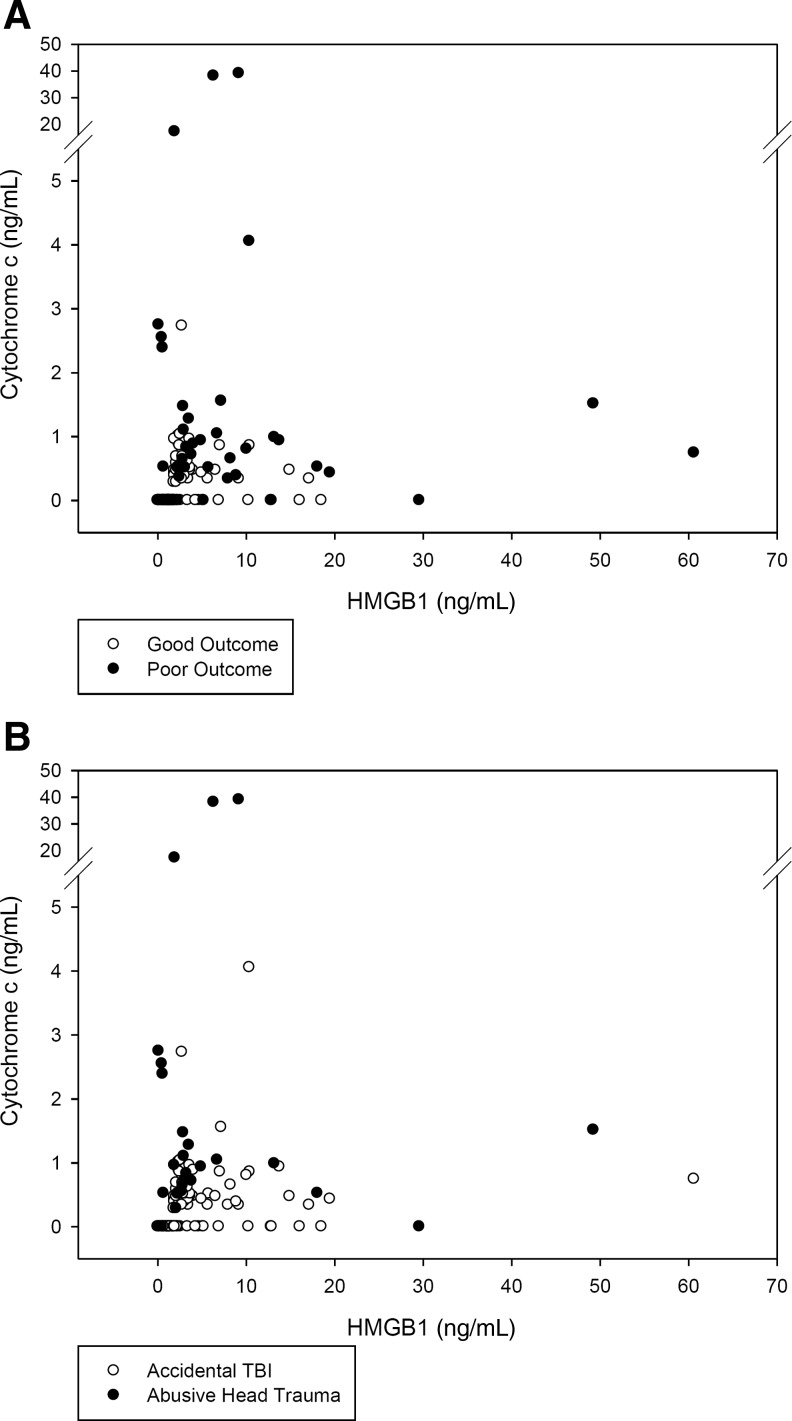
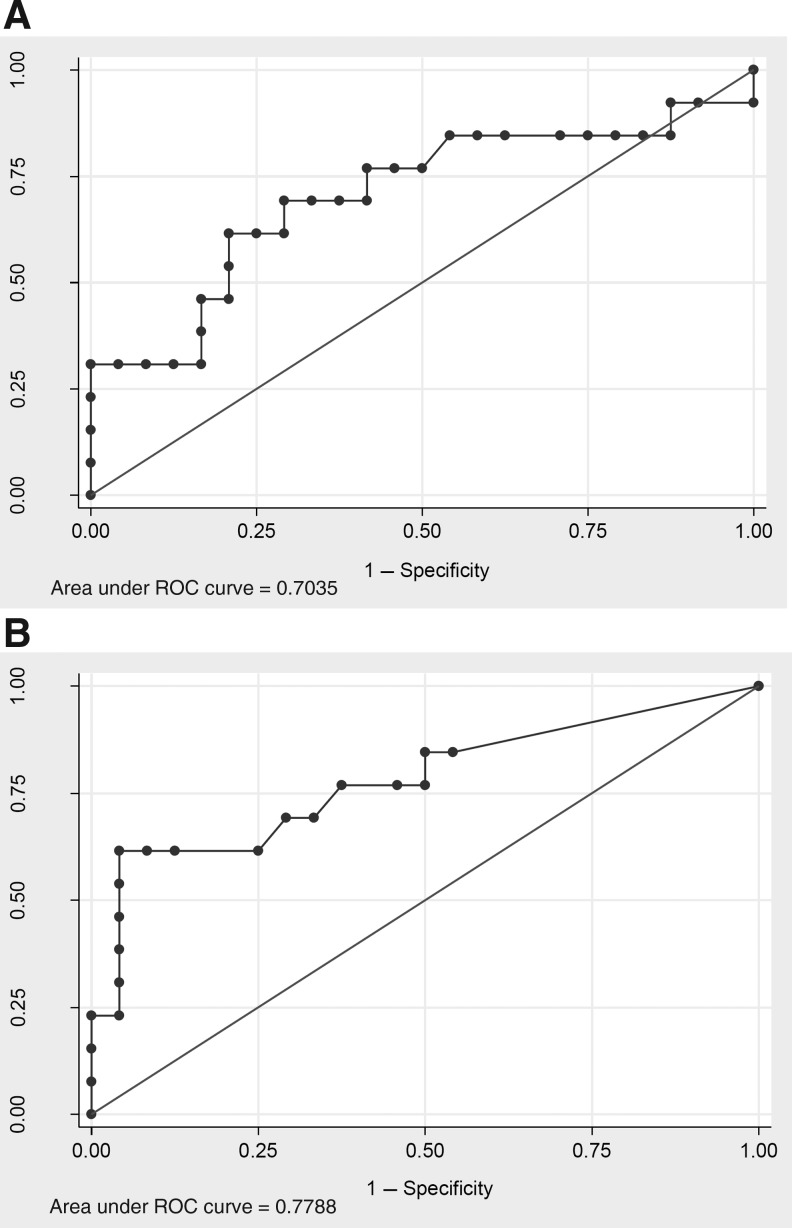
High-mobility group box 1 (HMGB1) is a ubiquitous nuclear protein that is passively released from damaged and necrotic cells, and actively released from immune cells. In contrast, cytochrome c is released from mitochondria in apoptotic cells, and is considered a reliable biomarker of apoptosis. Thus, HMGB1 and cytochrome c may in part reflect the degree of necrosis and apoptosis present after traumatic brain injury (TBI), where both are felt to contribute to cell death and neurological morbidity. Ventricular cerebrospinal fluid (CSF) was obtained from children admitted to the intensive care unit (ICU) after TBI (n=37). CSF levels of HMGB1 and cytochrome c were determined at four time intervals (0-24 h, 25-48 h, 49-72 h, and>72 h after injury) using enzyme-linked immunosorbent assay (ELISA). Lumbar CSF from children without TBI served as controls (n=12). CSF HMGB1 levels were: control=1.78±0.29, 0-24 h=5.73±1.45, 25-48 h=5.16±1.73, 49-72 h=4.13±0.75,>72 h=3.80±0.90 ng/mL (mean±SEM). Peak HMGB1 levels were inversely and independently associated with favorable Glasgow Outcome Scale (GOS) scores at 6 mo (0.49 [0.24-0.97]; OR [5-95% CI]). CSF cytochrome c levels were: control=0.37±0.10, 0-24 h=0.69±0.15, 25-48 h=0.82±0.48, 49-72 h=1.52±1.08,>72 h=1.38±1.02 ng/mL (mean±SEM). Peak cytochrome c levels were independently associated with abusive head trauma (AHT; 24.29 [1.77-334.03]) and inversely and independently associated with favorable GOS scores (0.42 [0.18-0.99]). In conclusion, increased CSF levels of HMGB1 and cytochrome c were associated with poor outcome after TBI in infants and children. These data are also consistent with the designation of HMGB1 as a "danger signal." Distinctly increased CSF cytochrome c levels in infants and children with AHT and poor outcome suggests that apoptosis may play an important role in this unique patient population.
Figures
References
-
- Adachi N. Hirota M. Hamaguchi M. Okamoto K. Watanabe K. Endo F. Serum cytochrome c level as a prognostic indicator in patients with systemic inflammatory response syndrome. Clin. Chim. Acta. 2004;342:127–136. - PubMed
-
- Adamsbaum C. Grabar S. Mejean N. Rey-Salmon C. Abusive head trauma: judicial admissions highlight violent and repetitive shaking. Pediatrics. 2010;126:546–555. - PubMed
-
- Adelson P.D. Bratton S.L. Carney N.A. Chesnut R.M. du Coudray H.E. Goldstein B. Kochanek P.M. Miller H.C. Partington M.D. Selden N.R. Warden C.R. Wright D.W. Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents. Pediatr. Crit. Care Med. 2003;4:S2–S75. - PubMed
-
- Adelson P.D. Ragheb J. Kanev P. Brockmeyer D. Beers S.R. Brown S.D. Cassidy L.D. Chang Y. Levin H. Phase II clinical trial of moderate hypothermia after severe traumatic brain injury in children. Neurosurgery. 2005;56:740–754. discussion 740–754. - PubMed
-
- Agrawal A. Schatz D.G. RAG1 and RAG2 form a stable postcleavage synaptic complex with DNA containing signal ends in V(D)J recombination. Cell. 1997;89:43–53. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
