

Hereditary angioedema (HAE) in children and adolescents--a consensus on therapeutic strategies
- PMID: 22543566
- PMCID: PMC3419830
- DOI: 10.1007/s00431-012-1726-4
Hereditary angioedema (HAE) in children and adolescents--a consensus on therapeutic strategies
Abstract
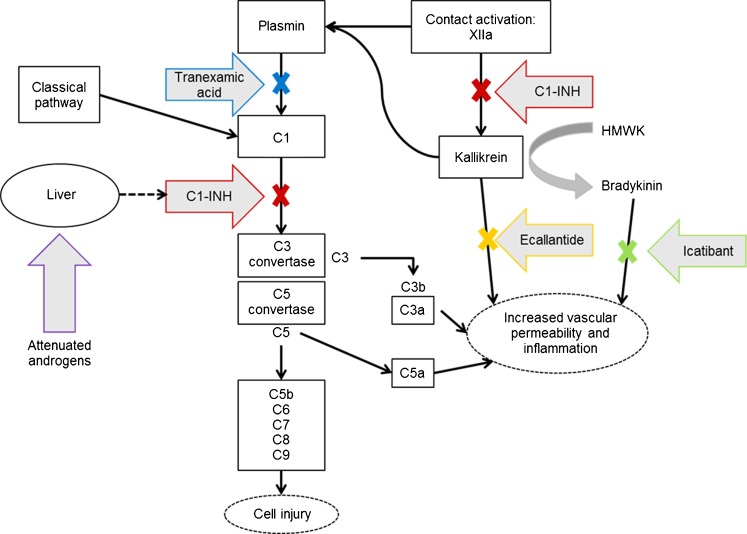
Hereditary angioedema due to C1 inhibitor (C1 esterase inhibitor) deficiency (types I and II HAE-C1-INH) is a rare disease that usually presents during childhood or adolescence with intermittent episodes of potentially life-threatening angioedema. Diagnosis as early as possible is important to avoid ineffective therapies and to properly treat swelling attacks. At a consensus meeting in June 2011, pediatricians and dermatologists from Germany, Austria, and Switzerland reviewed the currently available literature, including published international consensus recommendations for HAE therapy across all age groups. Published recommendations cannot be unconditionally adopted for pediatric patients in German-speaking countries given the current approval status of HAE drugs. This article provides an overview and discusses drugs available for HAE therapy, their approval status, and study results obtained in adult and pediatric patients. Recommendations for developing appropriate treatment strategies in the management of HAE in pediatric patients in German-speaking countries are provided.Conclusion Currently, plasma-derived C1 inhibitor concentrate is considered the best available option for the treatment of acute HAE-C1-INH attacks in pediatric patients in German-speaking countries, as well as for short-term and long-term prophylaxis.
Figures
References
-
- Bork K, Hardt J, Staubach-Renz P, Witzke G. Risk of laryngeal edema and facial swellings after tooth extraction in patients with hereditary angioedema with and without prophylaxis with C1 inhibitor concentrate: a retrospective study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112:58–64. doi: 10.1016/j.tripleo.2011.02.034. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
