

Acetabular tilt correlates with acetabular version and coverage in hip dysplasia
- PMID: 22544668
- PMCID: PMC3441999
- DOI: 10.1007/s11999-012-2370-z
Acetabular tilt correlates with acetabular version and coverage in hip dysplasia
Abstract
Background: The rotational position of the acetabulum to the pelvis (acetabular tilt) may influence acetabular version and coverage of the femoral head. To date, the pathologic significance of acetabular tilt in hip dysplasia is unknown.
Questions/purposes: We determined whether acetabular tilt in hip dysplasia is different from that in normal hips and whether this correlates with acetabular version and coverage.
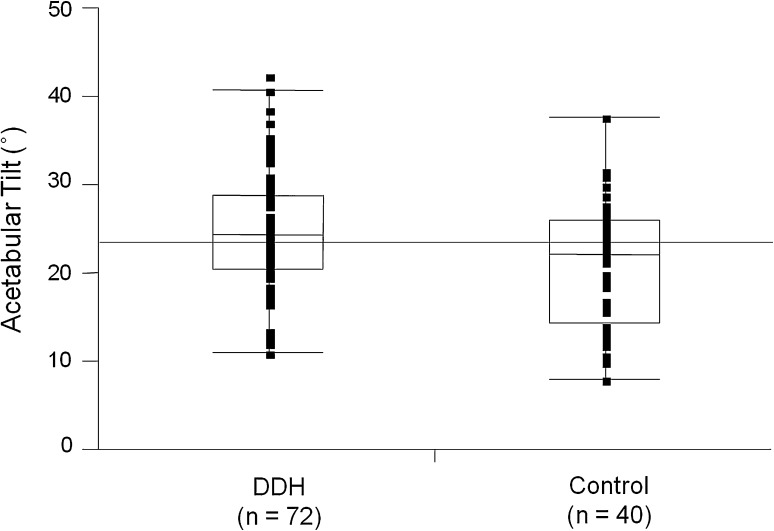
Methods: We measured the acetabular tilt angle on the lateral view of three-dimensional pelvic CT images of 40 patients (72 hips) with hip dysplasia. Forty normal hips from 40 patients were used as controls. The acetabular sector angle was measured as an index for acetabular coverage of the femoral head.
Results: The mean acetabular tilt angle was increased in dysplastic hips compared with controls. In dysplastic hips, a posteriorly rotated acetabulum (increased acetabular tilt) was associated with increased acetabular anteversion and with decreased anterior and anterosuperior acetabular coverage. No correlation was found in controls. In dysplastic hips with a posterior acetabular deficiency, the acetabulum was rotated anteriorly (decreased acetabular tilt) compared with hips with anterior and lateral deficiencies.
Conclusions: We observed a correlation between the rotational position of the acetabulum in the pelvis with acetabular version and coverage in hip dysplasia. Our observations confirmed anterior rotation of the acetabular fragment during periacetabular osteotomies is an anatomically reasonable maneuver for hips with anterolateral acetabular deficiencies, while the maneuver can exacerbate posterior coverage and should be avoided in hips with a posterior acetabular deficiency.
Level of evidence: Level IV, diagnostic study. See the Guidelines for Authors for a complete description of levels of evidence.
Figures





References
-
- Anda S, Svenningsen S, Dale LG, Benum P. The acetabular sector angle of the adult hip determined by computed tomography. Acta Radiol Diagn (Stockh). 1986;27:443–447. - PubMed
-
- Azuma H, Taneda H, Igarashi H, Fukuoka M. Preoperative and postoperative assessment of rotational acetabular osteotomy for dysplastic hips in children by three-dimensional surface reconstruction computed tomography imaging. J Pediatr Orthop. 1990;10:33–38. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
