

Worldwide patterns of bronchodilator responsiveness: results from the Burden of Obstructive Lung Disease study
- PMID: 22544896
- PMCID: PMC3402754
- DOI: 10.1136/thoraxjnl-2011-201445
Worldwide patterns of bronchodilator responsiveness: results from the Burden of Obstructive Lung Disease study
Abstract
Rationale: Criteria for a clinically significant bronchodilator response (BDR) are mainly based on studies in patients with obstructive lung diseases. Little is known about the BDR in healthy general populations, and even less about the worldwide patterns.
Methods: 10 360 adults aged 40 years and older from 14 countries in North America, Europe, Africa and Asia participated in the Burden of Obstructive Lung Disease study. Spirometry was used before and after an inhaled bronchodilator to determine the distribution of the BDR in population-based samples of healthy non-smokers and individuals with airflow obstruction.
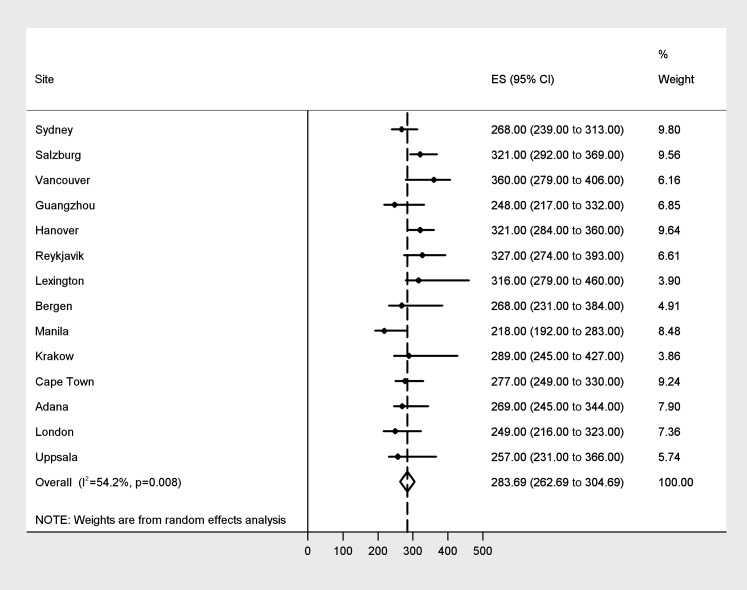
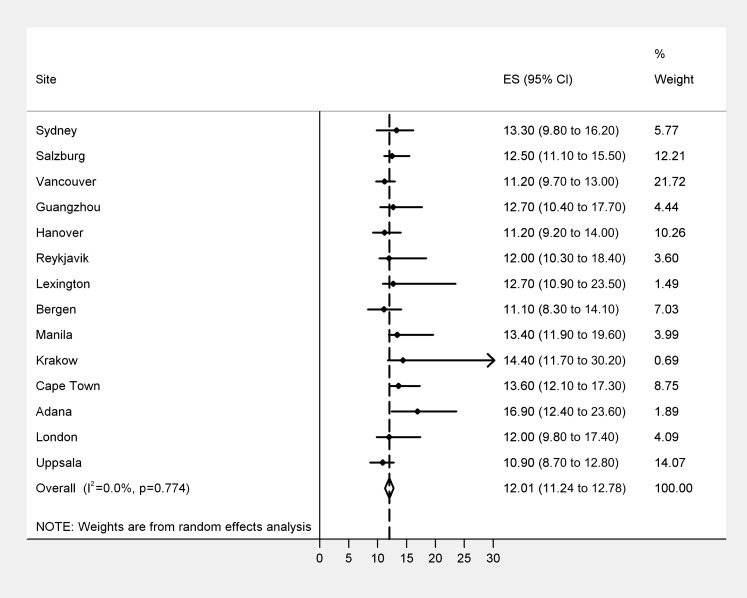
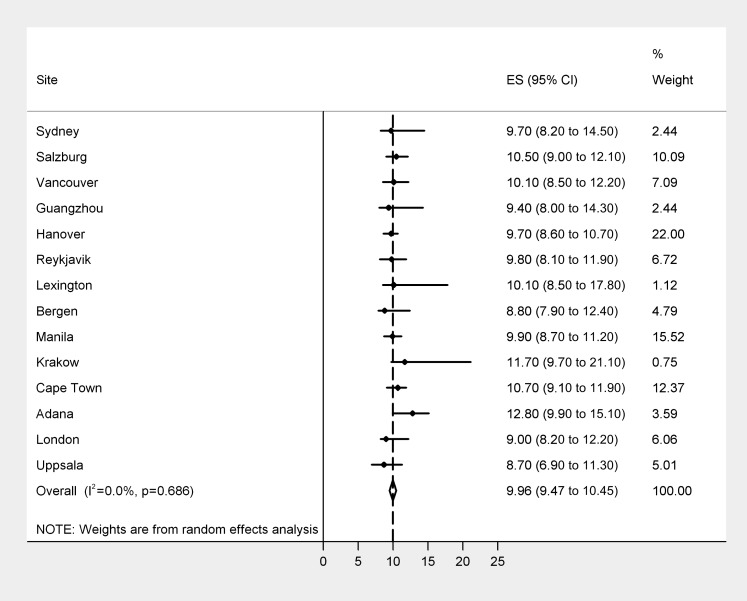
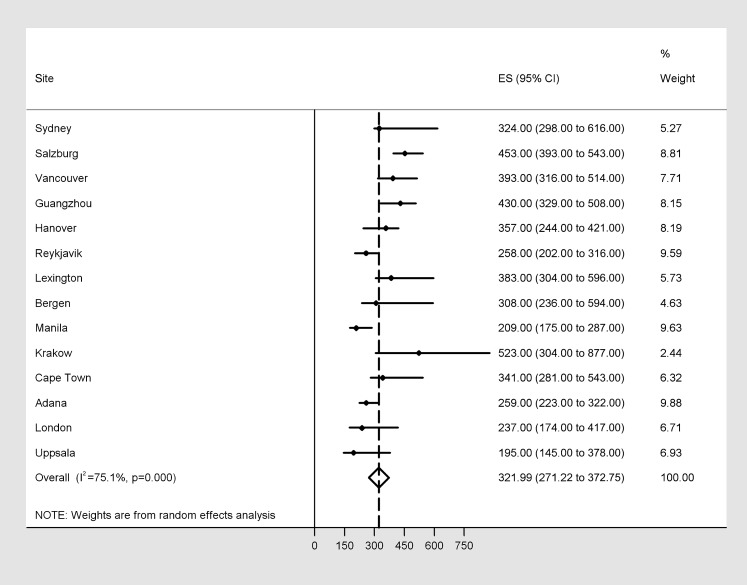
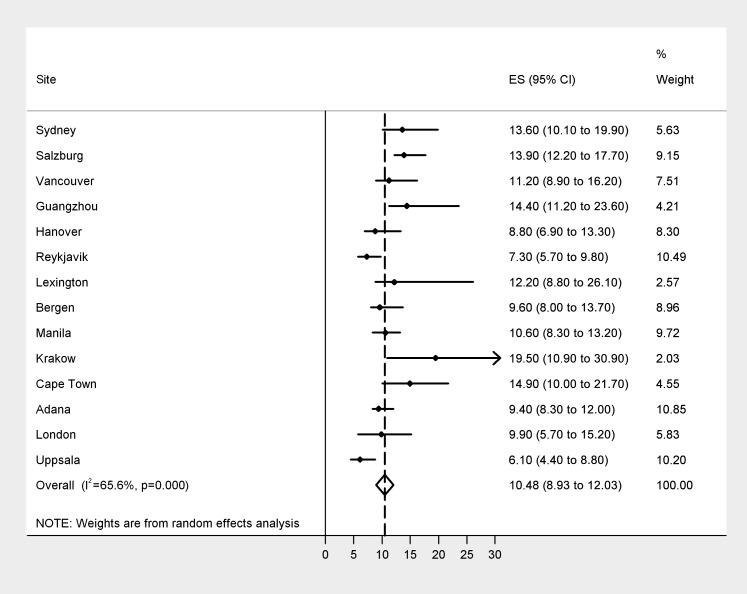
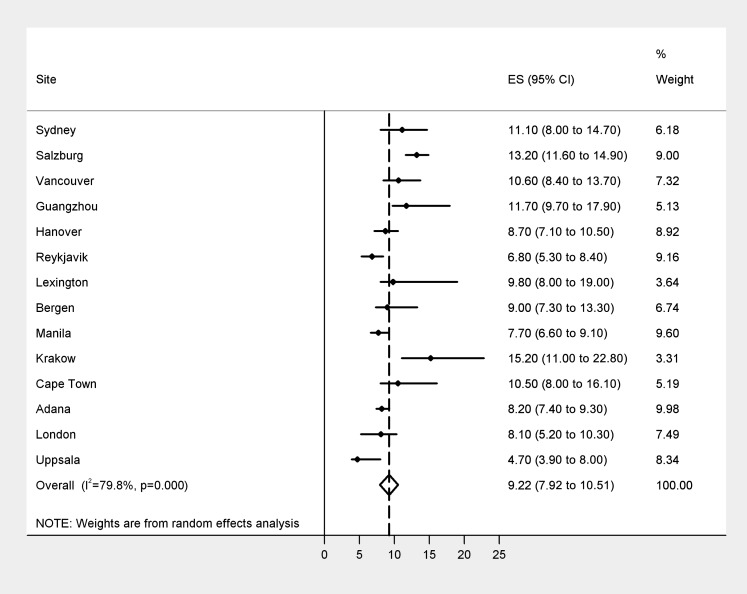
Results: In 3922 healthy never smokers, the weighted pooled estimate of the 95th percentiles (95% CI) for bronchodilator response were 284 ml (263 to 305) absolute change in forced expiratory volume in 1 s from baseline (ΔFEV(1)); 12.0% (11.2% to 12.8%) change relative to initial value (%ΔFEV(1i)); and 10.0% (9.5% to 10.5%) change relative to predicted value (%ΔFEV(1p)). The corresponding mean changes in forced vital capacity (FVC) were 322 ml (271 to 373) absolute change from baseline (ΔFVC); 10.5% (8.9% to 12.0%) change relative to initial value (ΔFVC(i)); and 9.2% (7.9% to 10.5%) change relative to predicted value (ΔFVC(p)). The proportion who exceeded the above threshold values in the subgroup with spirometrically defined Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage 2 and higher (FEV(1)/FVC <0.7 and FEV(1)% predicted <80%) were 11.1%, 30.8% and 12.9% respectively for the FEV(1)-based thresholds and 22.6%, 28.6% and 22.1% respectively for the FVC-based thresholds.
Conclusions: The results provide reference values for bronchodilator responses worldwide that confirm guideline estimates for a clinically significant level of BDR in bronchodilator testing.
Conflict of interest statement
Figures
Comment in
-
Bronchodilator responsiveness: interpret with caution.Thorax. 2012 Aug;67(8):667-8. doi: 10.1136/thoraxjnl-2012-201966. Epub 2012 Jun 12. Thorax. 2012. PMID: 22693176 No abstract available.
References
-
- Dompeling E, van Schayck CP, Molema J, et al. A comparison of six different ways of expressing the bronchodilating response in asthma and COPD: reproducibility and dependence of prebronchodilator FEV1. Eur Respir J 1992;5:975–81 - PubMed
-
- Nicklaus TM, Burgin WW, Jr, Taylor JR. Spirometric tests to diagnose suspected asthma. Am Rev Respir Dis 1969;100:153–9 - PubMed
-
- Tashkin DP, Celli B, Decramer M, et al. Bronchodilator responsiveness in patients with COPD. Eur Respir J 2008;31:742–50 - PubMed
-
- Anthonisen NR, Lindgren PG, Tashkin DP, et al. Bronchodilator response in the lung health study over 11 yrs. Eur Respir J 2005;26:45–51 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical