

Cost effectiveness analysis of clinically driven versus routine laboratory monitoring of antiretroviral therapy in Uganda and Zimbabwe
- PMID: 22545079
- PMCID: PMC3335836
- DOI: 10.1371/journal.pone.0033672
Cost effectiveness analysis of clinically driven versus routine laboratory monitoring of antiretroviral therapy in Uganda and Zimbabwe
Abstract
Background: Despite funding constraints for treatment programmes in Africa, the costs and economic consequences of routine laboratory monitoring for efficacy and toxicity of antiretroviral therapy (ART) have rarely been evaluated.
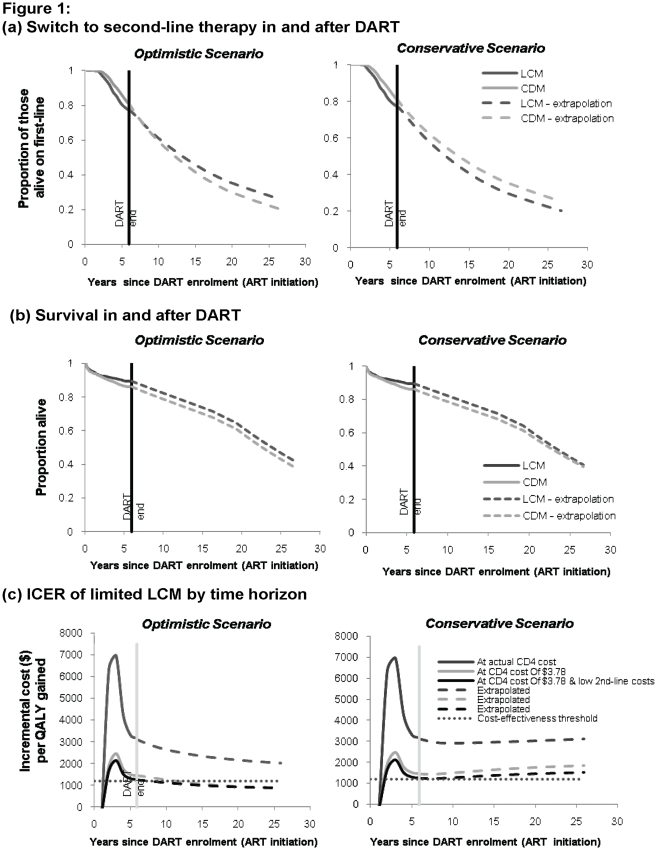
Methods: Cost-effectiveness analysis was conducted in the DART trial (ISRCTN13968779). Adults in Uganda/Zimbabwe starting ART were randomised to clinically-driven monitoring (CDM) or laboratory and clinical monitoring (LCM); individual patient data on healthcare resource utilisation and outcomes were valued with primary economic costs and utilities. Total costs of first/second-line ART, routine 12-weekly CD4 and biochemistry/haematology tests, additional diagnostic investigations, clinic visits, concomitant medications and hospitalisations were considered from the public healthcare sector perspective. A Markov model was used to extrapolate costs and benefits 20 years beyond the trial.
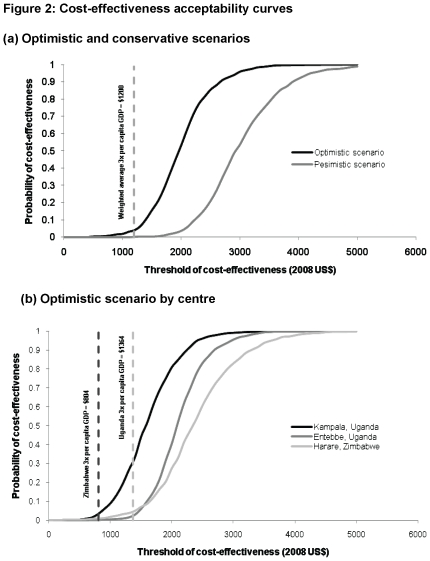
Results: 3316 (1660LCM;1656CDM) symptomatic, immunosuppressed ART-naive adults (median (IQR) age 37 (32,42); CD4 86 (31,139) cells/mm(3)) were followed for median 4.9 years. LCM had a mean 0.112 year (41 days) survival benefit at an additional mean cost of $765 [95%CI:685,845], translating into an adjusted incremental cost of $7386 [3277,dominated] per life-year gained and $7793 [4442,39179] per quality-adjusted life year gained. Routine toxicity tests were prominent cost-drivers and had no benefit. With 12-weekly CD4 monitoring from year 2 on ART, low-cost second-line ART, but without toxicity monitoring, CD4 test costs need to fall below $3.78 to become cost-effective (<3xper-capita GDP, following WHO benchmarks). CD4 monitoring at current costs as undertaken in DART was not cost-effective in the long-term.
Conclusions: There is no rationale for routine toxicity monitoring, which did not affect outcomes and was costly. Even though beneficial, there is little justification for routine 12-weekly CD4 monitoring of ART at current test costs in low-income African countries. CD4 monitoring, restricted to the second year on ART onwards, could be cost-effective with lower cost second-line therapy and development of a cheaper, ideally point-of-care, CD4 test.
Conflict of interest statement
Figures
References
-
- Gilks CF, Crowley S, Ekpini R, Perriens J, Souteyrand Y, et al. The WHO public health approach to antiretroviral treatment against HIV in resource-limited settings. Lancet. 2006;368:505–510. - PubMed
-
- World Health Organization. Progress report 2010: 1–150; 2010. Towards universal access: scaling up priority HIV/AIDS interventions in the health sector. pp. 1–150.
-
- World Bank. The global economic crisis and HIV prevention and treatment programmes; vulnerabilities and impact. 2009. pp. 1–40.
-
- Kenyon C, Skordis J, Boulle A, Pillay K. The ART of rationing–the need for a new approach to rationing health interventions. S Afr Med J. 2003;93:56–60. - PubMed
-
- Kent DM, McGrath D, Ioannidis JPA. Suitable monitoring approaches to antiretroviral therapy in resource-poor settings: setting the research agenda. Clinical Infectious Diseases. 2003;37:S13–24. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
