

Follow-up imaging to detect recurrence of surgically treated pediatric arteriovenous malformations
- PMID: 22546027
- PMCID: PMC3484378
- DOI: 10.3171/2012.1.PEDS11453
Follow-up imaging to detect recurrence of surgically treated pediatric arteriovenous malformations
Abstract
Object: The true postoperative incidence of arteriovenous malformation (AVM) recurrence in the pediatric population remains largely unreported. Some literature suggests that delayed imaging studies should be obtained at 6 months to 1 year after negative findings on a postoperative angiogram. The aim of this study was to describe the timing of AVM recurrences after resection and the neuroimaging modalities on which the recurrences were detected.
Methods: This study was performed in a retrospective cohort of all pediatric patients treated surgically for AVM resection by a single neurosurgeon between 2005 and 2010. Patients were followed after resection with MR angiography (MRA) or conventional angiography, when possible, at various time points. A visual scale for compactness of the initial AVM nidus was used, and the score was correlated with probability of recurrence after surgery.
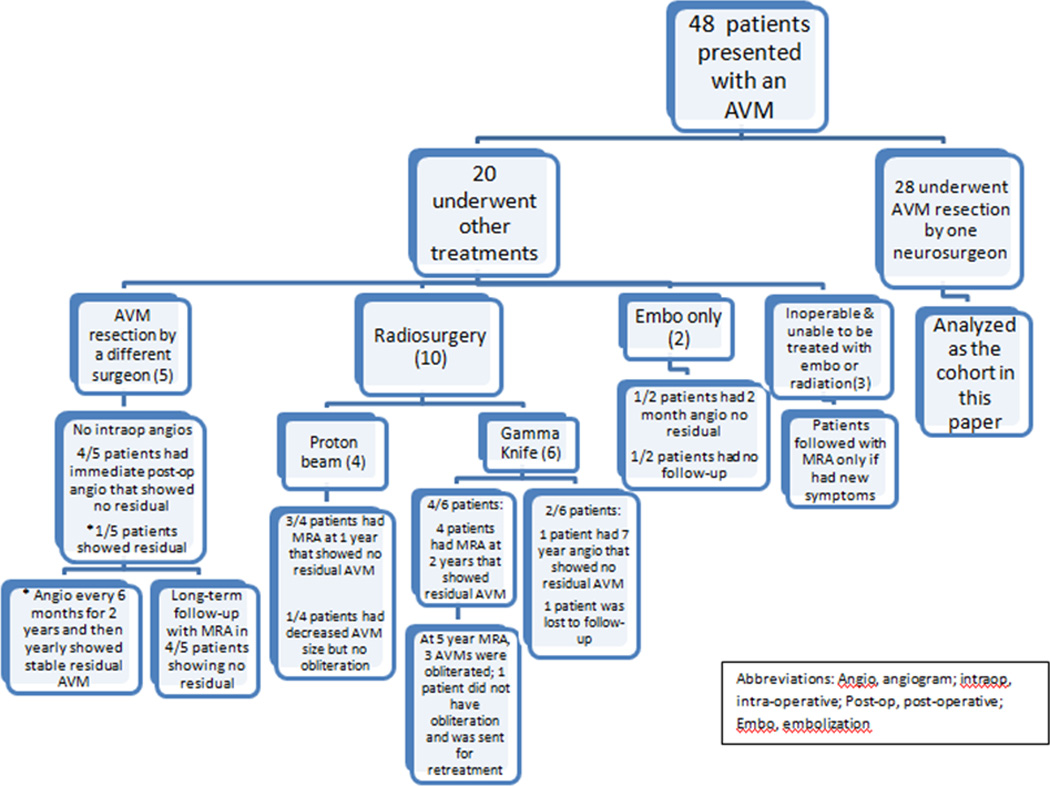
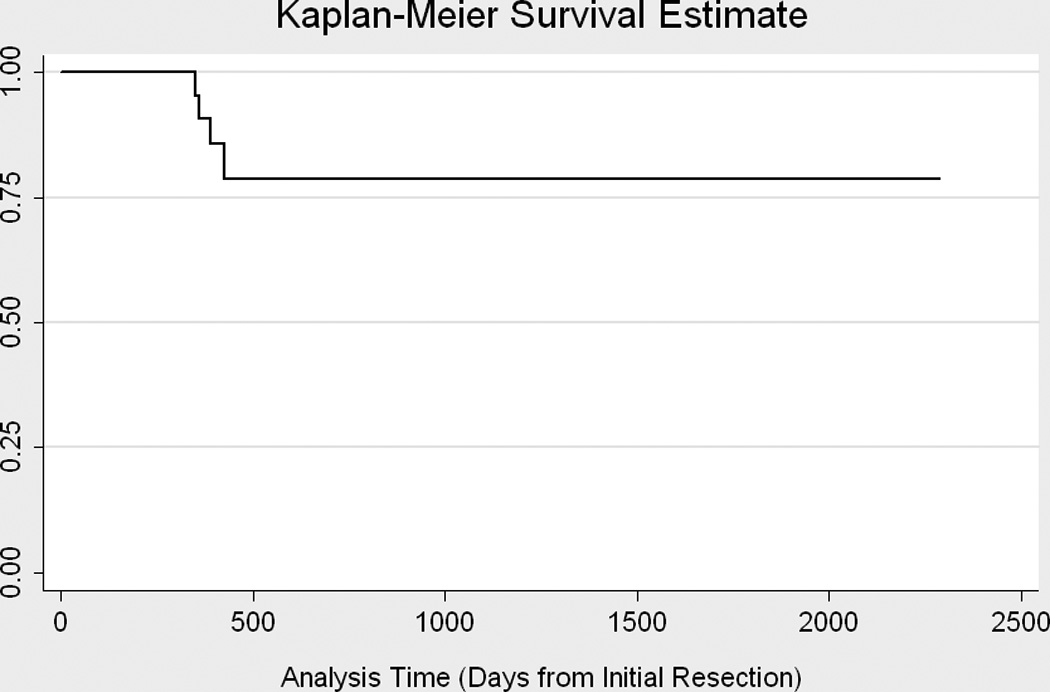
Results: A total of 28 patients (13 female, 15 male) underwent an AVM resection. In 18 patients (64.3%) an intraoperative angiogram was obtained. In 4 cases the intraoperative angiogram revealed residual AVM, and repeat resections were performed immediately. Recurrent AVMs were found in 4 children (14.3%) at 50, 51, 56, and 60 weeks after the initial resection. Recurrence risk was 0.08 per person-year. No patient with normal results on an angiogram obtained at 1 year developed a recurrence on either a 5-year angiogram or one obtained at 18 years of age. All patients with recurrence had a compactness score of 1 (diffuse AVM); a lower compactness score was associated with recurrence (p = 0.0003).
Conclusions: All recurrences in this cohort occurred less than 15 months from the initial resection. The authors recommend intraoperative angiography to help ensure complete resection at the time of the surgery. Follow-up vascular imaging is crucial for detecting recurrent AVMs, and conventional angiography is preferred because MRA can miss smaller AVMs. One-year follow-up imaging detected these recurrences, and no one who had negative results on an angiogram obtained at 1 year had a late recurrence. However, not all of the patients have been followed for 5 years or until 18 years of age, so longer follow-up is required for these patients. A lower compactness score predicted recurrent AVM in this cohort.
Conflict of interest statement
None of the authors has any disclosures or conflicts of interest.
Figures

References
-
- Ali MJ, Bendok BR, Rosenblatt S, Rose JE, Getch CC, Batjer HH. Recurrence of pediatric cerebral arteriovenous malformations after angiographically documented resection. Pediatr Neurosurg. 2003;39:32–38. - PubMed
-
- Andaluz N, Myseros JS, Sathi S, Crone KR, Tew JM., Jr Recurrence of cerebral arteriovenous malformations in children: report of two cases and review of the literature. Surg Neurol. 2004;62:324–330. discussion 330-321. - PubMed
-
- Bristol RE, Albuquerque FC, Spetzler RF, Rekate HL, McDougall CG, Zabramski JM. Surgical management of arteriovenous malformations in children. J Neurosurg. 2006;105:88–93. - PubMed
-
- Deruty R, Pelissou-Guyotat I, Amat D, Mottolese C, Bascoulergue Y, Turjman F, Gerard JP. Multidisciplinary treatment of cerebral arteriovenous malformations. Neurol Res. 1995;17:169–177. - PubMed
-
- Di Rocco C, Tamburrini G, Rollo M. Cerebral arteriovenous malformations in children. Acta Neurochir (Wien) 2000;142:145–156. discussion 156-148. - PubMed
Publication types
MeSH terms
Grants and funding
- 5R01HL090615-02/HL/NHLBI NIH HHS/United States
- R01 NS072338/NS/NINDS NIH HHS/United States
- R01 HL090615/HL/NHLBI NIH HHS/United States
- 1R21EY020662-01A1/EY/NEI NIH HHS/United States
- K12-NS049453/NS/NINDS NIH HHS/United States
- 1R15CA115464-01A2/CA/NCI NIH HHS/United States
- 1R01NS072338-01A1/NS/NINDS NIH HHS/United States
- R15 CA115464/CA/NCI NIH HHS/United States
- T32 NS007413/NS/NINDS NIH HHS/United States
- T32-NS007413/NS/NINDS NIH HHS/United States
- R21 EY020662/EY/NEI NIH HHS/United States
- K12 NS049453/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
