

Review
doi: 10.1186/cc11142.
Clinical review: the hospital of the future - building intelligent environments to facilitate safe and effective acute care delivery
Affiliations
- PMID: 22546172
- PMCID: PMC3681335
- DOI: 10.1186/cc11142
Item in Clipboard
Review
Clinical review: the hospital of the future - building intelligent environments to facilitate safe and effective acute care delivery
Crit Care.
.
Abstract
The translation of knowledge into rational care is as essential and pressing a task as the development of new diagnostic or therapeutic devices, and is arguably more important. The emerging science of health care delivery has identified the central role of human factor ergonomics in the prevention of medical error, omission, and waste. Novel informatics and systems engineering strategies provide an excellent opportunity to improve the design of acute care delivery. In this article, future hospitals are envisioned as organizations built around smart environments that facilitate consistent delivery of effective, equitable, and error-free care focused on patient-centered rather than provider-centered outcomes.
Figures
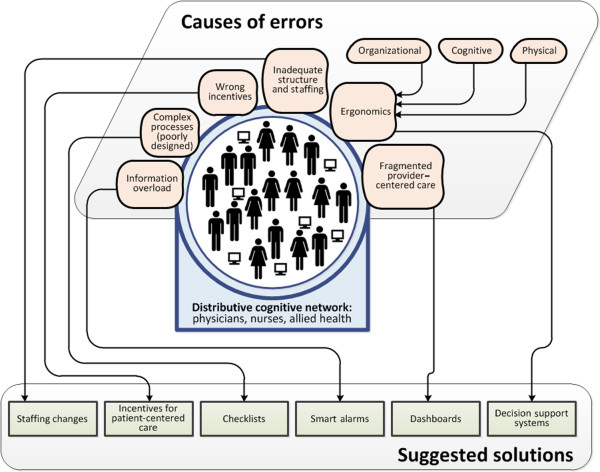
Challenges and opportunities for improving health care delivery in acute hospitals.
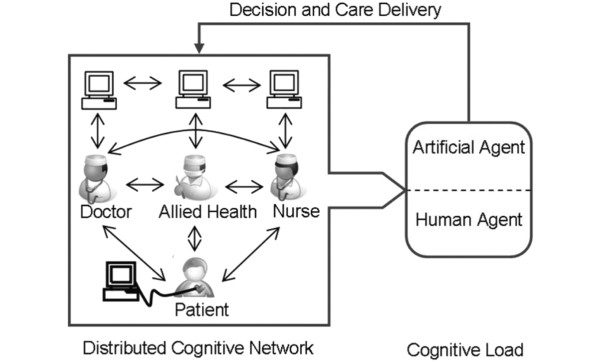
The distributed cognitive network - understanding how multidisciplinary teams deliver care in complex environments. A network of providers, utilizing a variety of environmental artifacts (data from electronic medical records, bedside monitors, to do lists from other providers, notes taken on rounds) make decisions and act upon them to deliver care to the patient. Understanding how that network functions, where its vulnerabilities lie and how it reacts to changes in the operational environment will facilitate the emergence of tools (organizational, decision support, smart alerts, novel user interfaces, and ambient intelligence applications) that improve the reliability, efficacy and safety of the care delivered to the bedside. In this illustration the artificial agent (health information technology-enabled decision supports, for example) act in co-operation with the human agents (nurses, doctors) to facilitate the development of a care plan. Modified from Figure 1a in [58].
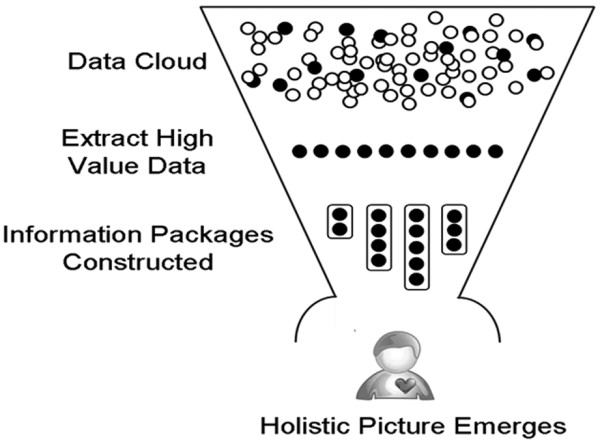
Cognitive science - understanding how health care providers make decisions and what motivates them to act. A greater understanding of how providers identify high value environmental data cues, incorporate them into mental models of patient states and develop a plan of care that can be acted upon by a multidisciplinary team is essential if we are to develop smart environments that support that activity. Reprinted from Figure 1b in [58].
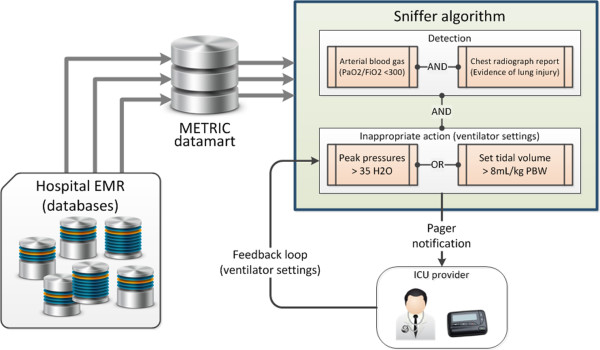
Smart environments alter system behaviors. Example of how a smart environment may be built upon an understanding of disease state and relevant provider actions (ventilator-induced lung injury is exacerbated by high tidal volumes), cognitive science (providers need information about the patient disease state and current ventilator settings to determine if a potentially injurious ventilator strategy is being applied to a patient), health care informatics (where do the data for each of the decision-making cues reside and how can the sensitivity and specificity of a smart alert algorithm be optimized to the condition of interest?), and ergonomics (who should be notified and how the message should be delivered - paged alerts are disruptive but very effective if they are meaningful to the recipient). EMR, electronic medical record; METRIC, multidisciplinary epidemiology and translational research in intensive care; PBW, predicted body weight.
References
-
- Kohn K, Corrigan J, Donaldson M. To Err is Human: Building a Safer Health System. Vol. 16. Washington, DC: National Academy Press; 1999. pp. 26–48. - PubMed
-
- Kohn L, Donaldson MS. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; 1999. - PubMed
-
- Haynes AB, Weiser TG, Berry WR, Lipsitz SR, Breizat AH, Dellinger EP, Herbosa T, Joseph S, Kibatala PL, Lapitan MC, Merry AF, Moorthy K, Reznick RK, Taylor B, Gawande AA. Safe Surgery Saves Lives Study Group. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med. 2009;16:491–499. doi: 10.1056/NEJMsa0810119. - DOI - PubMed
-
- Levy MM, Pronovost PJ, Dellinger RP, Townsend S, Resar RK, Clemmer TP, Ramsay G. Sepsis change bundles: converting guidelines into meaningful change in behavior and clinical outcome. Crit Care Med. 2004;16(11 Suppl):S595–597. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
