

Nebulized anticoagulants for acute lung injury - a systematic review of preclinical and clinical investigations
- PMID: 22546487
- PMCID: PMC3681399
- DOI: 10.1186/cc11325
Nebulized anticoagulants for acute lung injury - a systematic review of preclinical and clinical investigations
Abstract
Background: Data from interventional trials of systemic anticoagulation for sepsis inconsistently suggest beneficial effects in case of acute lung injury (ALI). Severe systemic bleeding due to anticoagulation may have offset the possible positive effects. Nebulization of anticoagulants may allow for improved local biological availability and as such may improve efficacy in the lungs and lower the risk of systemic bleeding complications.
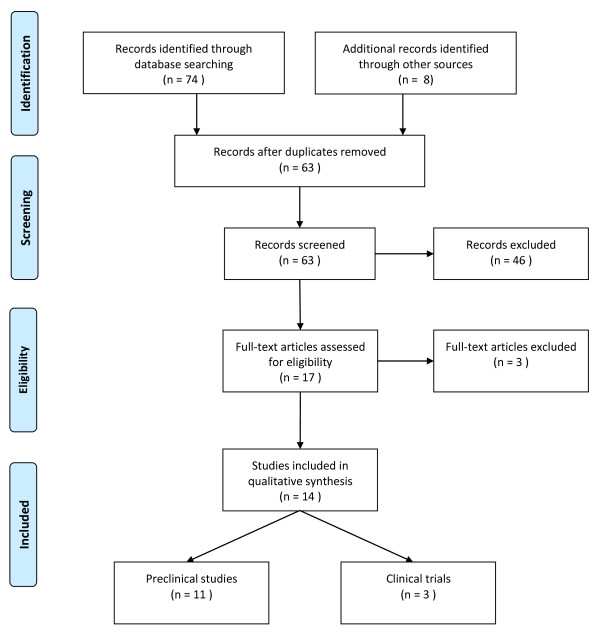
Method: We performed a systematic review of preclinical studies and clinical trials investigating the efficacy and safety of nebulized anticoagulants in the setting of lung injury in animals and ALI in humans.
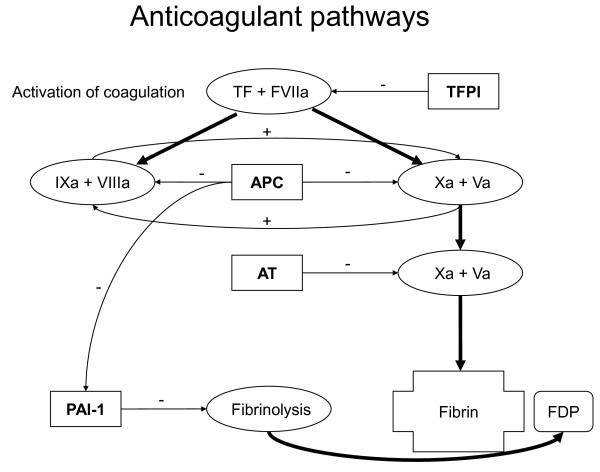
Results: The efficacy of nebulized activated protein C, antithrombin, heparin and danaparoid has been tested in diverse animal models of direct (for example, pneumonia-, intra-pulmonary lipopolysaccharide (LPS)-, and smoke inhalation-induced lung injury) and indirect lung injury (for example, intravenous LPS- and trauma-induced lung injury). Nebulized anticoagulants were found to have the potential to attenuate pulmonary coagulopathy and frequently also inflammation. Notably, nebulized danaparoid and heparin but not activated protein C and antithrombin, were found to have an effect on systemic coagulation. Clinical trials of nebulized anticoagulants are very limited. Nebulized heparin was found to improve survival of patients with smoke inhalation-induced ALI. In a trial of critically ill patients who needed mechanical ventilation for longer than two days, nebulized heparin was associated with a higher number of ventilator-free days. In line with results from preclinical studies, nebulization of heparin was found to have an effect on systemic coagulation, but without causing systemic bleedings.
Conclusion: Local anticoagulant therapy through nebulization of anticoagulants attenuates pulmonary coagulopathy and frequently also inflammation in preclinical studies of lung injury. Recent human trials suggest nebulized heparin for ALI to be beneficial and safe, but data are very limited.
Figures
References
-
- Gunther A, Mosavi P, Heinemann S, Ruppert C, Muth H, Markart P, Grimminger F, Walmrath D, Temmesfeld-Wollbruck B, Seeger W. Alveolar fibrin formation caused by enhanced procoagulant and depressed fibrinolytic capacities in severe pneumonia. Comparison with the acute respiratory distress syndrome. Am J Respir Crit Care Med. 2000;16:454–462. - PubMed
-
- Schultz MJ, Haitsma JJ, Zhang H, Slutsky AS. Pulmonary coagulopathy as a new target in therapeutic studies of acute lung injury or pneumonia - a review. Crit Care Med. 2006;16:871–877. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
