

Predicting acute and persistent neuropathy associated with oxaliplatin
- PMID: 22547012
- PMCID: PMC4080710
- DOI: 10.1097/COC.0b013e318246b50d
Predicting acute and persistent neuropathy associated with oxaliplatin
Abstract
Objectives: We sought to predict oxaliplatin-associated peripheral neuropathy during modified FOLFOX6 (mFOLFOX6) therapy.
Methods: Equal numbers of male and female patients with previously untreated, primary or recurrent colorectal cancer were followed through a first course of mFOLFOX6 with 85 mg/m² oxaliplatin every 2 weeks. Accounting for correlation among a subject's cycle, logistic regression estimated per cycle risk of acute (under 14 d) and persistent (14 d or more) neuropathy. Proportional hazards regression predicted time to persistent neuropathy.
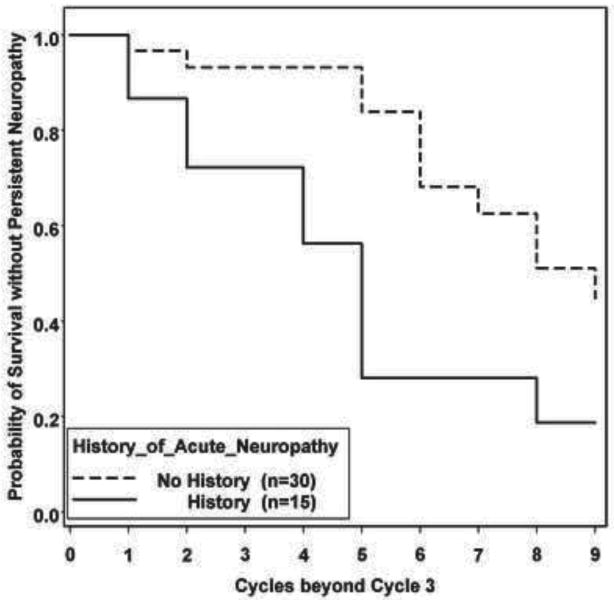
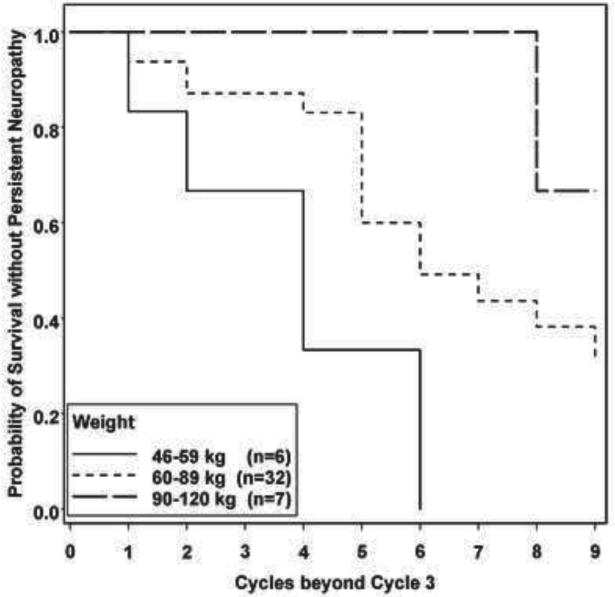
Results: Among mFOLFOX6 recipients (n = 50, age 58.9 ± 10.1 y), 36% received concomitant bevacizumab. Of the total number of cycles, 94.2% (422/448) were evaluable. Most (84%) subjects reported neuropathy at least once; 74% reported acute and 48% reported persistent symptoms. On multivariate analysis, risk factors shared by acute and persistent neuropathy were body surface area >2.0, acute neuropathy in a past cycle, and lower body weight. In addition, risk of acute neuropathy decreased with age (adjusted for renal function and winter season), whereas risk of persistent neuropathy increased with cumulative dose of oxaliplatin and persistent neuropathy in a past cycle. Concomitant bevacizumab was not a risk factor when administered in stage IV disease but was associated with persistent neuropathy when administered experimentally in stage III. Females had no increased risk of either form of neuropathy. After 3 cycles, weight, body surface area, and prior acute neuropathy predicted time to persistent neuropathy.
Conclusions: Routinely available clinical factors predict acute and persistent neuropathy associated with oxaliplatin. When validated, the proposed prognostic score for persistent neuropathy can help clinicians counsel patients about chemotherapy.
Figures


References
-
- Park SB, Goldstein D, Lin CSY, et al. Acute abnormalities of sensory nerve function associated with oxaliplatin-induced neurotoxicity. J Clin Oncol. 2009;27:1243–1249. - PubMed
-
- Park SB, Lin CS, Krishnan AV, et al. Oxaliplatin-induced neurotoxicity: changes in axonal excitability precede development of neuropathy. Brain. 2009;132:2712–2723. - PubMed
-
- Gamelin E, Gamelin L, Bossi L, et al. Clinical aspects and molecular basis of oxaliplatin neurotoxicity: current management and development of preventive measures. Semin Oncol. 2002;29:21–33. - PubMed
-
- Krishnan AV, Goldstein D, Friedlander M, et al. Oxaliplatin-induced neurotoxicity and the development of neuropathy. Muscle Nerve. 2005;32:51–60. - PubMed
-
- Pietrangeli A, Leandri M, Terzoli E, et al. Persistence of high-dose oxaliplatin-induced neuropathy at long-term follow-up. Eur Neurol. 2006;56:13–16. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
