

The role of adiponectin in cancer: a review of current evidence
- PMID: 22547160
- PMCID: PMC3410224
- DOI: 10.1210/er.2011-1015
The role of adiponectin in cancer: a review of current evidence
Abstract
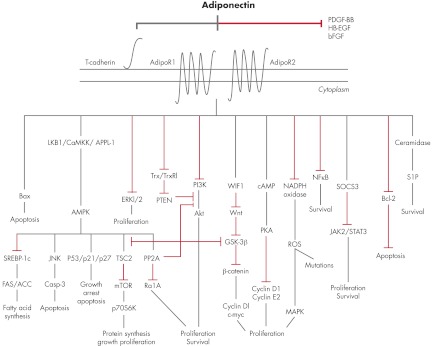
Excess body weight is associated not only with an increased risk of type 2 diabetes and cardiovascular disease (CVD) but also with various types of malignancies. Adiponectin, the most abundant protein secreted by adipose tissue, exhibits insulin-sensitizing, antiinflammatory, antiatherogenic, proapoptotic, and antiproliferative properties. Circulating adiponectin levels, which are determined predominantly by genetic factors, diet, physical activity, and abdominal adiposity, are decreased in patients with diabetes, CVD, and several obesity-associated cancers. Also, adiponectin levels are inversely associated with the risk of developing diabetes, CVD, and several malignancies later in life. Many cancer cell lines express adiponectin receptors, and adiponectin in vitro limits cell proliferation and induces apoptosis. Recent in vitro studies demonstrate the antiangiogenic and tumor growth-limiting properties of adiponectin. Studies in both animals and humans have investigated adiponectin and adiponectin receptor regulation and expression in several cancers. Current evidence supports a role of adiponectin as a novel risk factor and potential diagnostic and prognostic biomarker in cancer. In addition, either adiponectin per se or medications that increase adiponectin levels or up-regulate signaling pathways downstream of adiponectin may prove to be useful anticancer agents. This review presents the role of adiponectin in carcinogenesis and cancer progression and examines the pathophysiological mechanisms that underlie the association between adiponectin and malignancy in the context of a dysfunctional adipose tissue in obesity. Understanding of these mechanisms may be important for the development of preventive and therapeutic strategies against obesity-associated malignancies.
Figures
References
-
- Hubert HB, Feinleib M, McNamara PM, Castelli WP. 1983. Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of participants in the Framingham Heart Study. Circulation 67:968–977 - PubMed
-
- Mokdad AH, Ford ES, Bowman BA, Dietz WH, Vinicor F, Bales VS, Marks JS. 2003. Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA 289:76–79 - PubMed
-
- Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. 2006. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA 295:1549–1555 - PubMed
-
- Ogden CL, Yanovski SZ, Carroll MD, Flegal KM. 2007. The epidemiology of obesity. Gastroenterology 132:2087–2102 - PubMed
-
- Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. 2008. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet 371:569–578 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
