

Considerations in the rationale, design and methods of the Strategic Timing of AntiRetroviral Treatment (START) study
- PMID: 22547421
- PMCID: PMC3664112
- DOI: 10.1177/1740774512440342
Considerations in the rationale, design and methods of the Strategic Timing of AntiRetroviral Treatment (START) study
Abstract
Background: Untreated human immunodeficiency virus (HIV) infection is characterized by progressive depletion of CD4+ T lymphocyte (CD4) count leading to the development of opportunistic diseases (acquired immunodeficiency syndrome (AIDS)), and more recent data suggest that HIV is also associated with an increased risk of serious non-AIDS (SNA) diseases including cardiovascular, renal, and liver diseases and non-AIDS-defining cancers. Although combination antiretroviral treatment (ART) has resulted in a substantial decrease in morbidity and mortality in persons with HIV infection, viral eradication is not feasible with currently available drugs. The optimal time to start ART for asymptomatic HIV infection is controversial and remains one of the key unanswered questions in the clinical management of HIV-infected individuals.
Purpose: In this article, we outline the rationale and methods of the Strategic Timing of AntiRetroviral Treatment (START) study, an ongoing multicenter international trial designed to assess the risks and benefits of initiating ART earlier than is currently practiced. We also describe some of the challenges encountered in the design and implementation of the study and how these challenges were addressed.
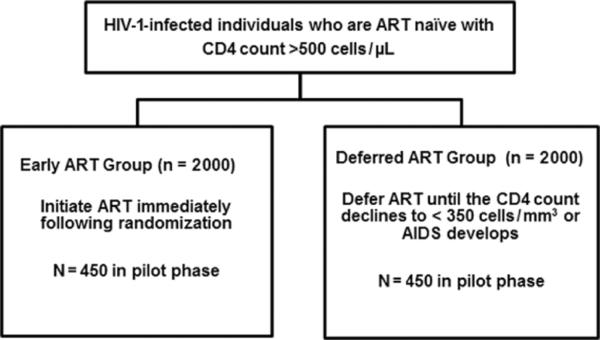
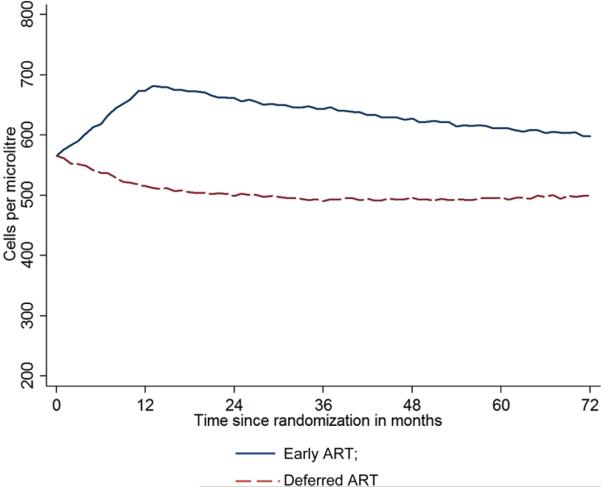
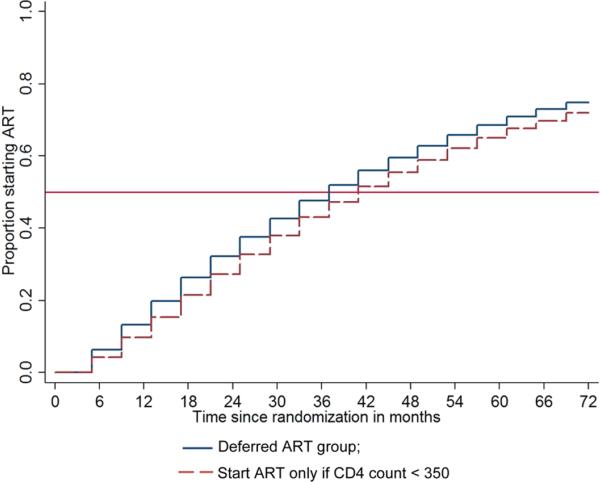
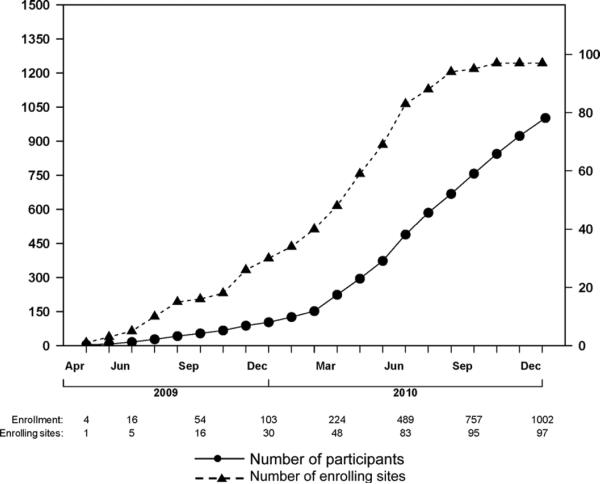
Methods: A total of 4000 study participants who are HIV type 1 (HIV-1) infected, ART naïve with CD4 count > 500 cells/µL are to be randomly allocated in a 1:1 ratio to start ART immediately (early ART) or defer treatment until CD4 count is <350 cells/µL (deferred ART) and followed for a minimum of 3 years. The primary outcome is time to AIDS, SNA, or death. The study had a pilot phase to establish feasibility of accrual, which was set as the enrollment of at least 900 participants in the first year.
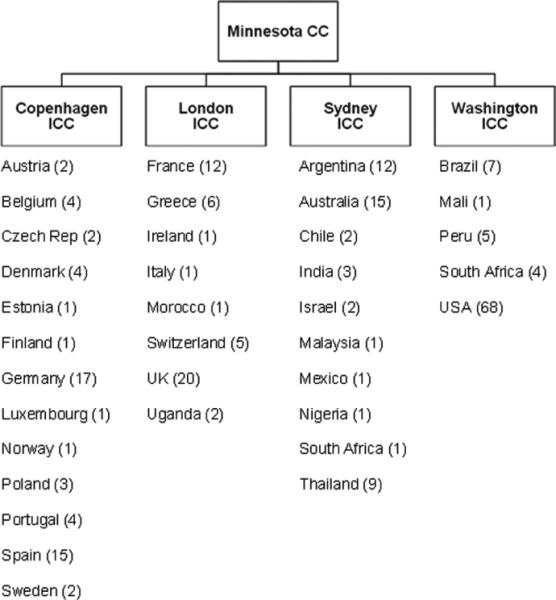
Results: Challenges encountered in the design and implementation of the study included the limited amount of data on the risk of a major component of the primary endpoint (SNA) in the study population, changes in treatment guidelines when the pilot phase was well underway, and the complexities of conducting the trial in a geographically wide population with diverse regulatory requirements. With the successful completion of the pilot phase, more than 1000 participants from 100 sites in 23 countries have been enrolled. The study will expand to include 237 sites in 36 countries to reach the target accrual of 4000 participants.
Conclusions: START is addressing one of the most important questions in the clinical management of ART. The randomization provided a platform for the conduct of several substudies aimed at increasing our understanding of HIV disease and the effects of antiretroviral therapy beyond the primary question of the trial. The lessons learned from its design and implementation will hopefully be of use to future publicly funded international trials.
Figures
References
-
- Bhaskaran K, Hamouda O, Sannes M, et al. Changes in the risk of death after HIV seroconversion compared with mortality in the general population. JAMA. 2008;300(2):5–9. - PubMed
-
- Mocroft A, Ledergerber B, Katlama C, et al. Decline in the AIDS and death rates in the EuroSIDA study: An observational study. Lancet. 2003;362:22–29. - PubMed
-
- European AIDS Clinical Society (EACS) Guidelines for the clinical management and treatment of HIV infected adults in Europe. Version 5. Dec, 2009. [(accessed 22 March 2012)]. Available at: http://www.europeanaidsclinicalsociety.org/images/stories/EACS-Pdf/versi....
-
- Gazzard BG, on behalf of the BHIVA Treatment Guidelines Writing Group British HIV Association guidelines for the treatment of HIV-1-infected adults with antiretroviral therapy. HIV Med. 2008;9:563–608. - PubMed
-
- World Health Organisation [(accessed 1 October 2010)];Antiretroviral therapy for HIV infection in adults and adolescents – Recommendations for a public health approach 2010 revision. Available at: http://whqlibdoc.who.int/publications/2010/9789241599764_eng.pdf. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
