

Randomized phase II trial of erlotinib alone or with carboplatin and paclitaxel in patients who were never or light former smokers with advanced lung adenocarcinoma: CALGB 30406 trial
- PMID: 22547605
- PMCID: PMC3397694
- DOI: 10.1200/JCO.2011.40.1315
Randomized phase II trial of erlotinib alone or with carboplatin and paclitaxel in patients who were never or light former smokers with advanced lung adenocarcinoma: CALGB 30406 trial
Abstract
Purpose: Erlotinib is clinically effective in patients with non-small-cell lung cancer (NSCLC) who have adenocarcinoma, are never or limited former smokers, or have EGFR mutant tumors. We investigated the efficacy of erlotinib alone or in combination with chemotherapy in patients with these characteristics.
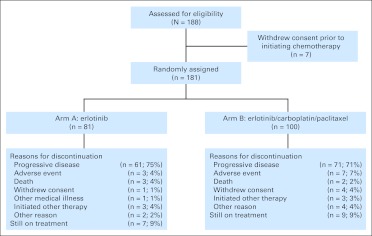
Patients and methods: Patients with advanced NSCLC (adenocarcinoma) who were epidermal growth factor receptor tyrosine kinase inhibitor and chemotherapy naive never or light former smokers (smokers of > 100 cigarettes and ≤ 10 pack years and quit ≥ 1 year ago) were randomly assigned to continuous erlotinib or in combination with carboplatin and paclitaxel (ECP) for six cycles followed by erlotinib alone. The primary end point was progression-free survival (PFS). Tissue collection was mandatory.
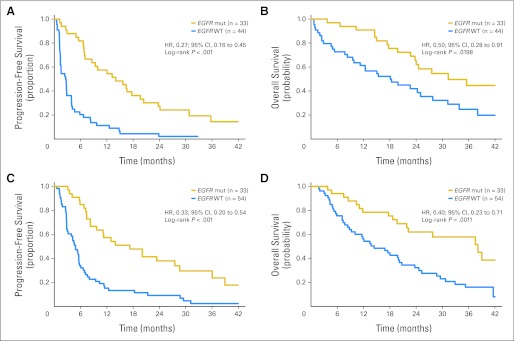
Results: PFS was similar (5.0 v 6.6 months; P = .1988) in patients randomly assigned to erlotinib alone (arm A; n = 81) or to ECP (arm B; n = 100). EGFR mutation analysis was possible in 91% (164 of 181) of patients, and EGFR mutations were detected in 40% (51 of 128) of never smokers and in 42% (15 of 36) of light former smokers. In arm A, response rate (70% v 9%), PFS (14.1 v 2.6 months), and overall survival (OS; 31.3 v 18.1 month) favored EGFR-mutant patients. In arm B, response rate (73% v 30%), PFS (17.2 v 4.8 months), and OS (38.1 v 14.4 months) favored EGFR-mutant patients. Incidence of grades 3 to 4 hematologic (2% v 49%; P < .001) and nonhematologic (24% v 52%; P < .001) toxicity was greater in patients treated with ECP.
Conclusion: Erlotinib and erlotinib plus chemotherapy have similar efficacy in clinically selected populations of patients with advanced NSCLC. EGFR mutations identify patients most likely to benefit.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures


Comment in
-
Method to our madness or madness in our methods? Pitfalls in trial methodology.J Clin Oncol. 2012 Jun 10;30(17):2025-7. doi: 10.1200/JCO.2011.41.4912. Epub 2012 Apr 30. J Clin Oncol. 2012. PMID: 22547587 No abstract available.
References
-
- Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Schiller JH, Harrington D, Belani CP, et al. Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N Engl J Med. 2002;346:92–98. - PubMed
-
- Shepherd FA, Rodrigues Pereira J, Ciuleanu T, et al. Erlotinib in previously treated non-small-cell lung cancer. N Engl J Med. 2005;353:123–132. - PubMed
-
- Paez JG, Jänne PA, Lee JC, et al. EGFR mutations in lung cancer: Correlation with clinical response to gefitinib therapy. Science. 2004;304:1497–1500. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
