

Risk score for predicting long-term mortality after coronary artery bypass graft surgery
- PMID: 22547673
- PMCID: PMC3422677
- DOI: 10.1161/CIRCULATIONAHA.111.055939
Risk score for predicting long-term mortality after coronary artery bypass graft surgery
Abstract
Background: No simplified bedside risk scores have been created to predict long-term mortality after coronary artery bypass graft surgery.
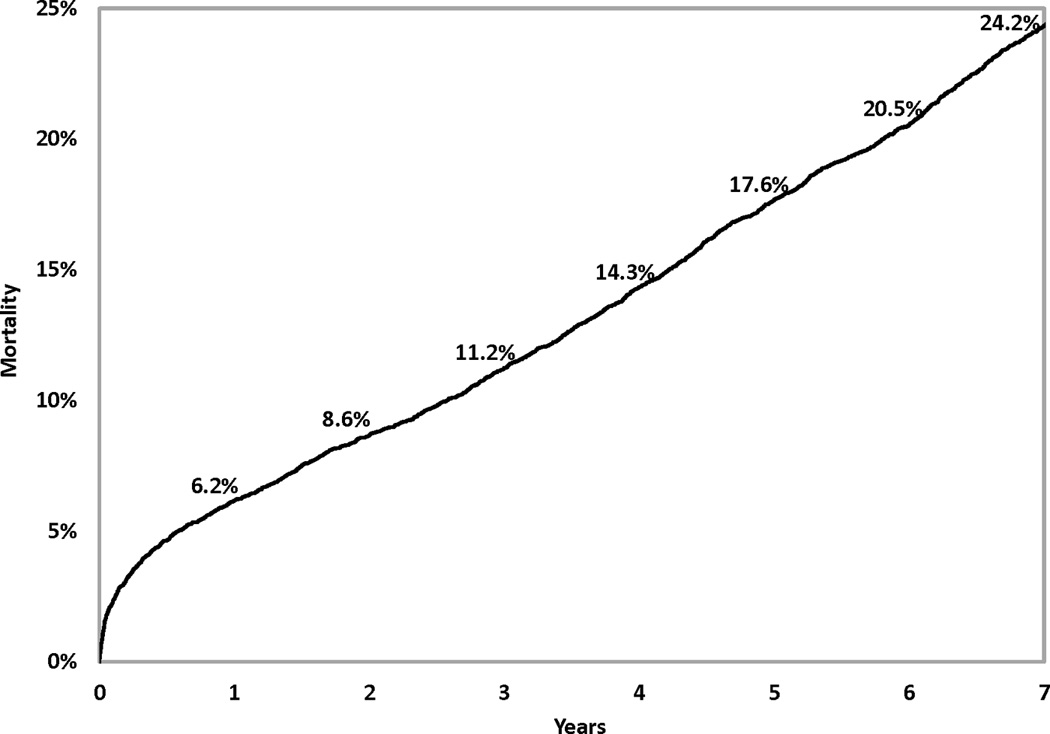
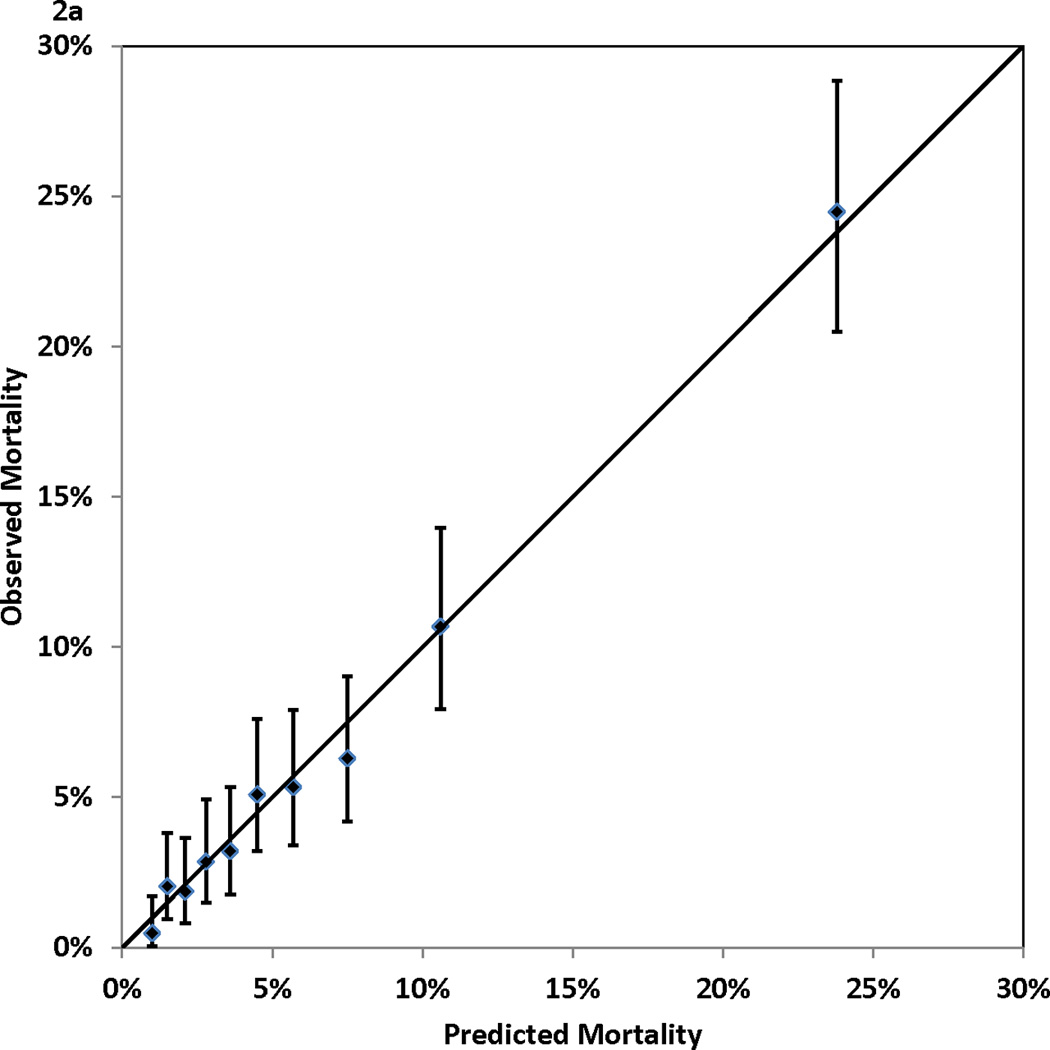
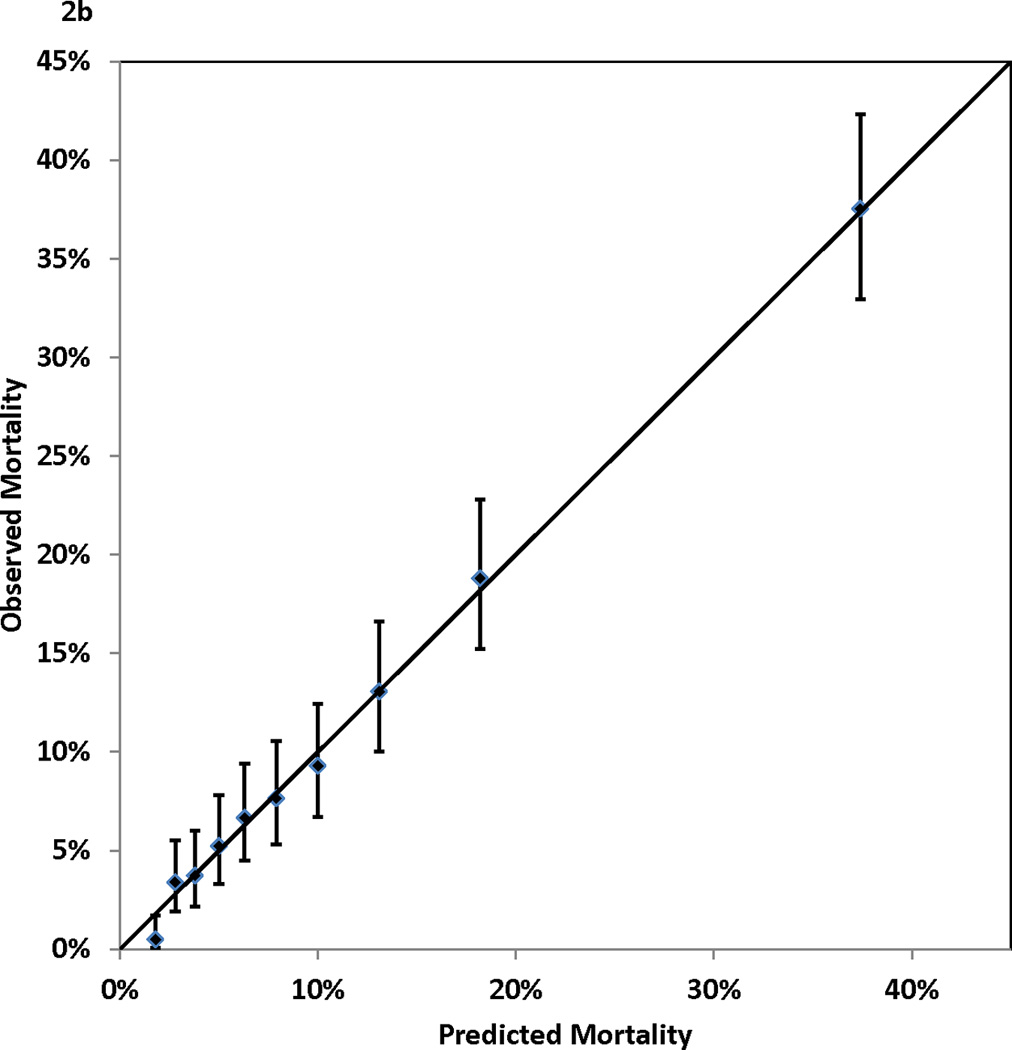
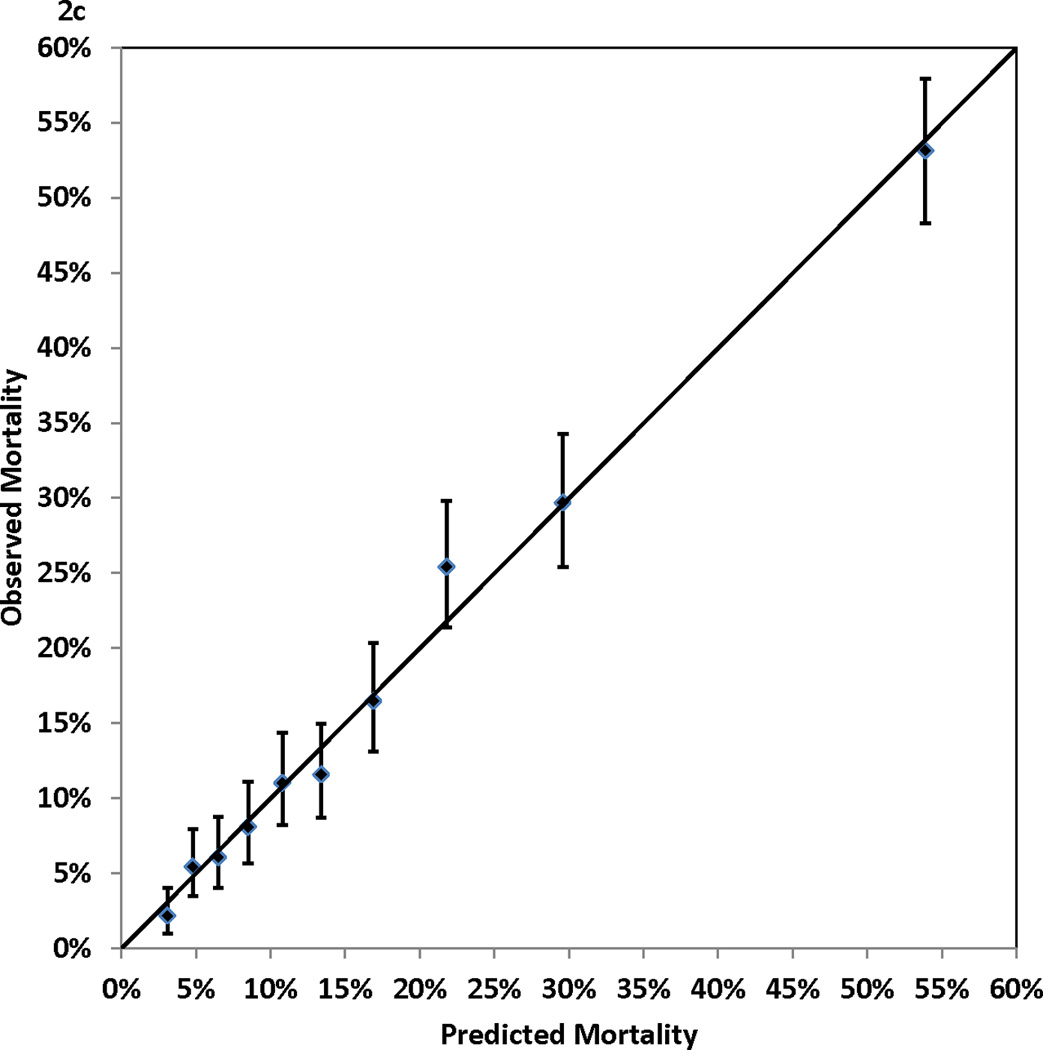
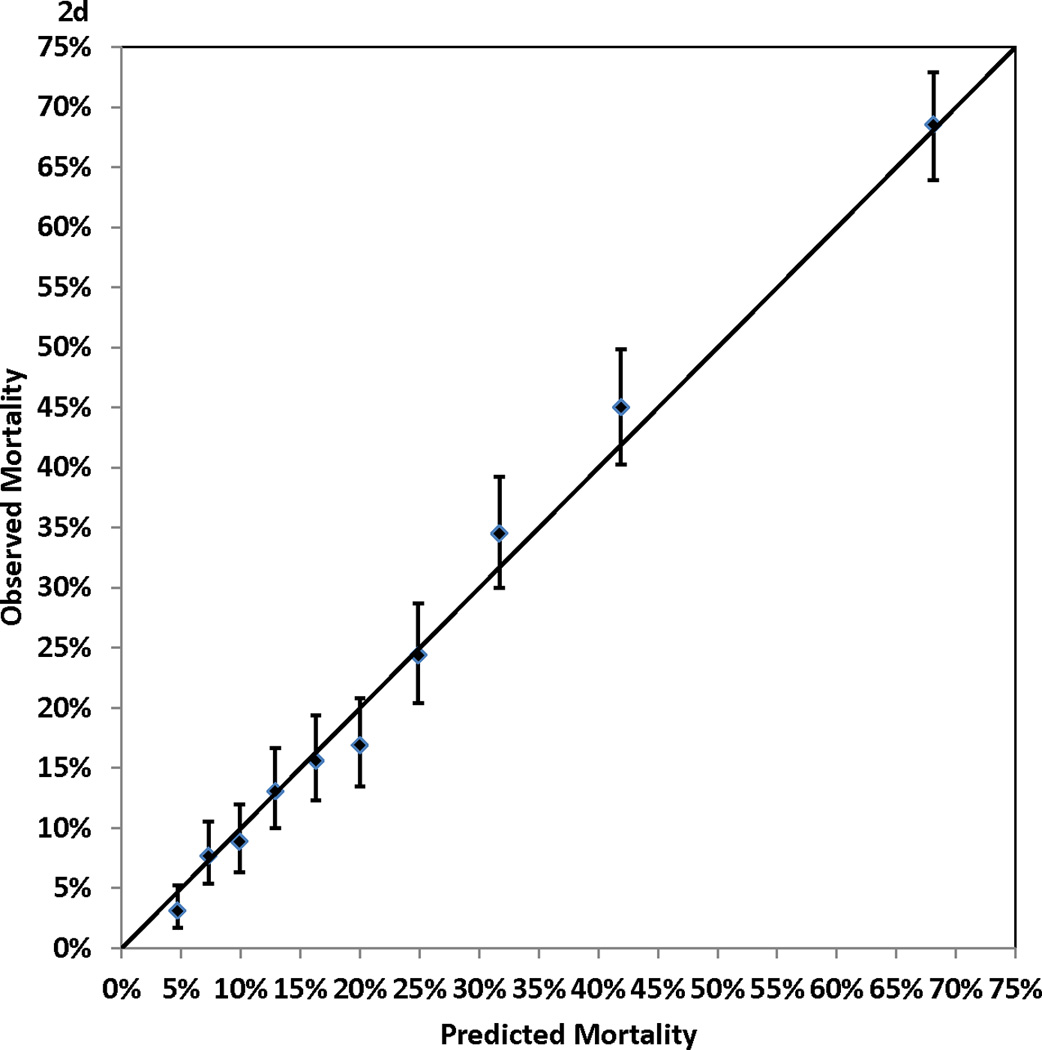
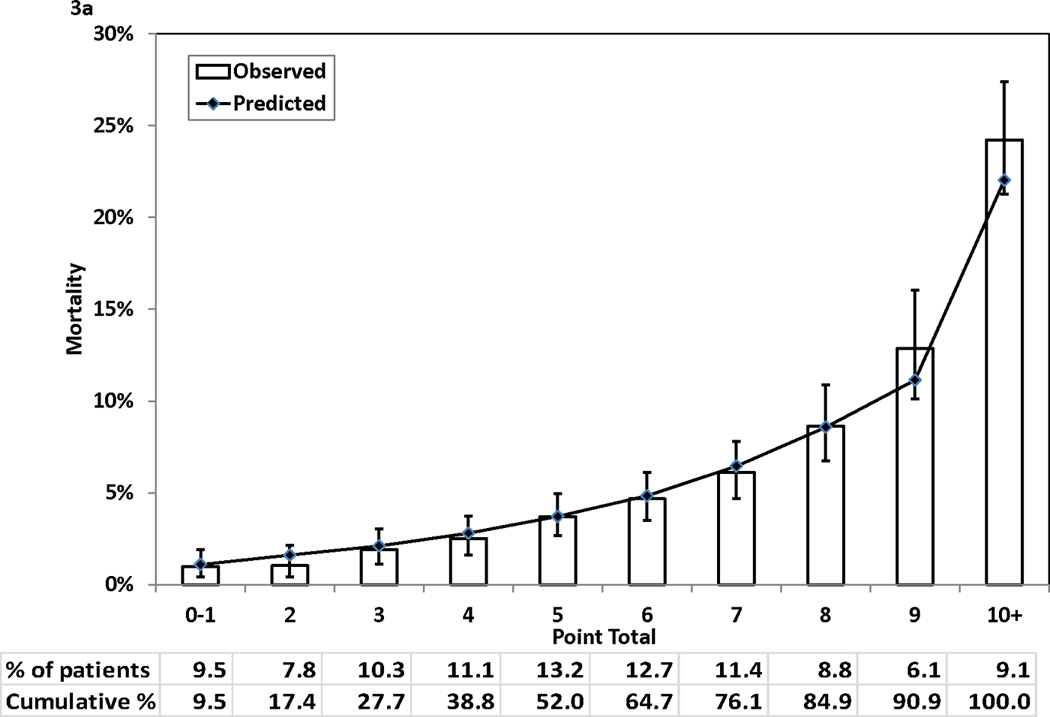
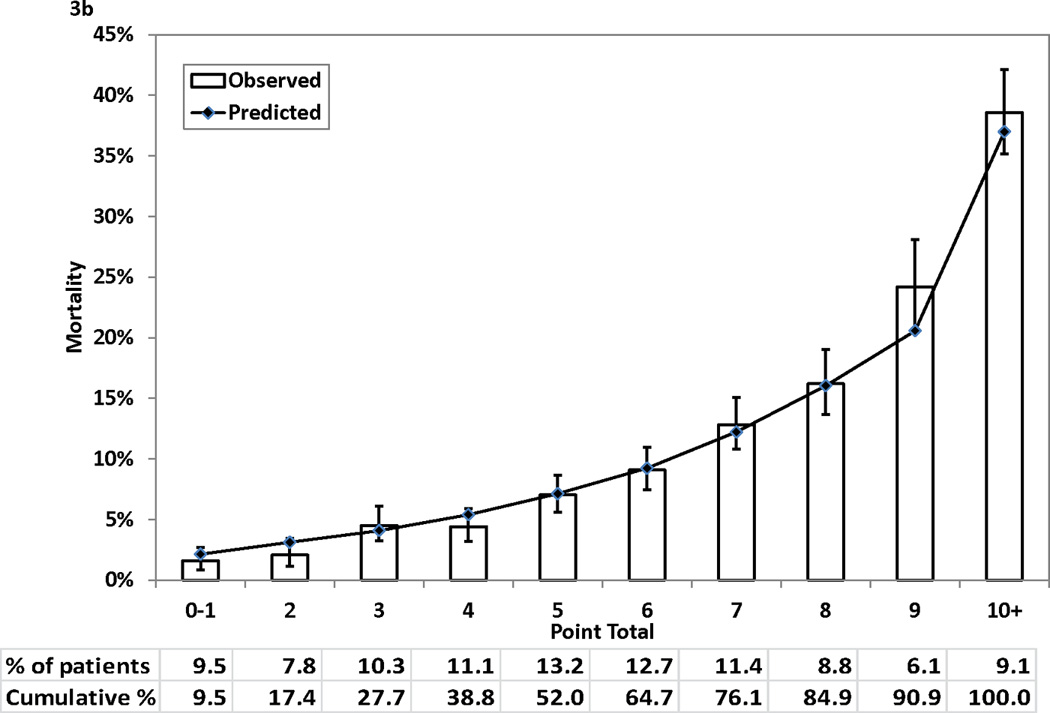
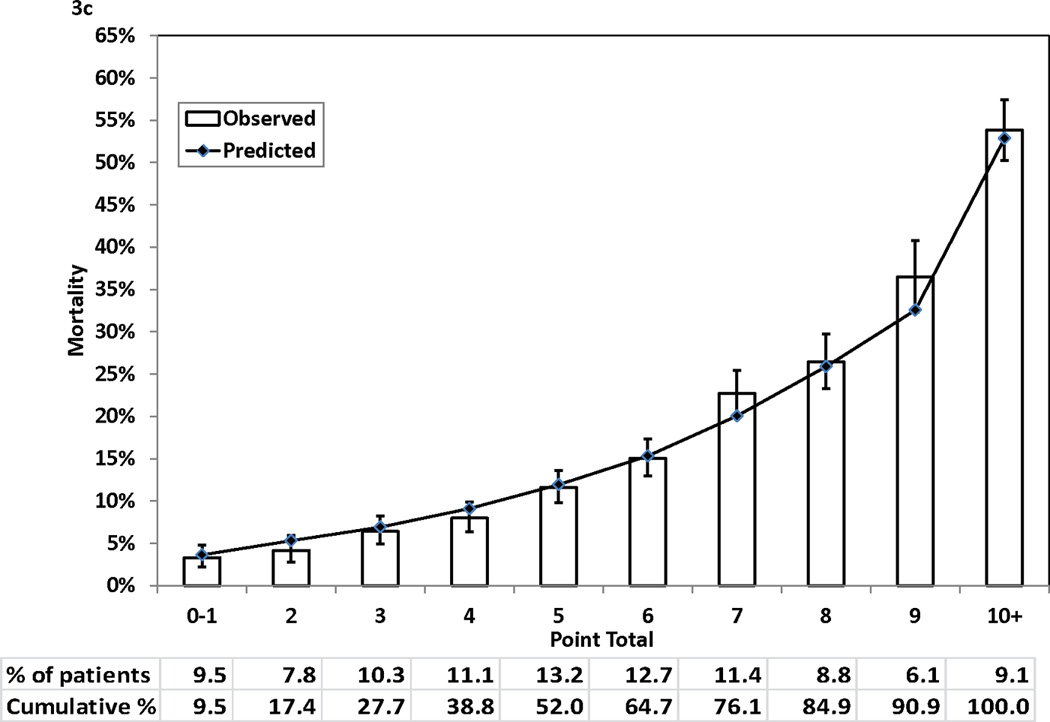
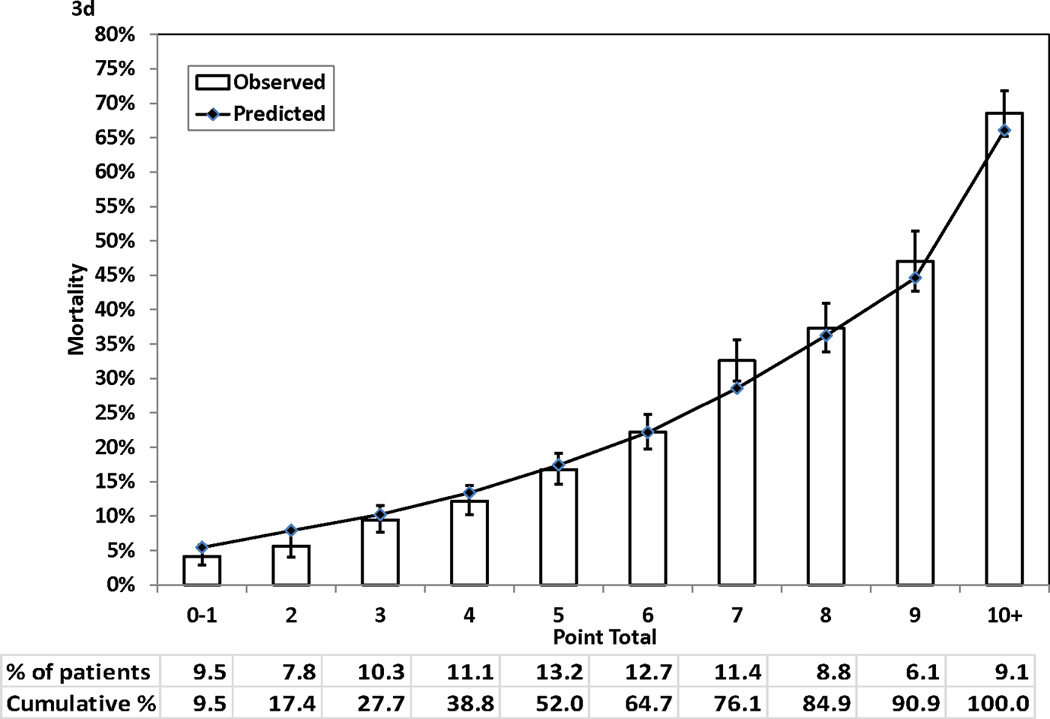
Methods and results: The New York State Cardiac Surgery Reporting System was used to identify 8597 patients who underwent isolated coronary artery bypass graft surgery in July through December 2000. The National Death Index was used to ascertain patients' vital statuses through December 31, 2007. A Cox proportional hazards model was fit to predict death after CABG surgery using preprocedural risk factors. Then, points were assigned to significant predictors of death on the basis of the values of their regression coefficients. For each possible point total, the predicted risks of death at years 1, 3, 5, and 7 were calculated. It was found that the 7-year mortality rate was 24.2 in the study population. Significant predictors of death included age, body mass index, ejection fraction, unstable hemodynamic state or shock, left main coronary artery disease, cerebrovascular disease, peripheral arterial disease, congestive heart failure, malignant ventricular arrhythmia, chronic obstructive pulmonary disease, diabetes mellitus, renal failure, and history of open heart surgery. The points assigned to these risk factors ranged from 1 to 7; possible point totals for each patient ranged from 0 to 28. The observed and predicted risks of death at years 1, 3, 5, and 7 across patient groups stratified by point totals were highly correlated.
Conclusion: The simplified risk score accurately predicted the risk of mortality after coronary artery bypass graft surgery and can be used for informed consent and as an aid in determining treatment choice.
Conflict of interest statement
Figures
Comment in
-
Mortality in coronary artery bypass grafting: what's next?Circulation. 2012 May 22;125(20):2409-11. doi: 10.1161/CIRCULATIONAHA.112.106856. Epub 2012 Apr 30. Circulation. 2012. PMID: 22547672 No abstract available.
References
-
- Higgins TL, Estafanous FG, Loop FD, Beck GJ, Blum JM, Paranandi L. Stratification of morbidity and mortality outcome by preoperative risk-factors in coronary-artery bypass patients - a clinical severity score. JAMA-J. Am. Med. Assoc. 1992;267:2344–2348. - PubMed
-
- Wouters SCW, Noyez L, Verheugt FWA, Brouwer R. Preoperative prediction of early mortality and morbidity in coronary bypass surgery. Cardiovasc. Surg. 2002;10:500–505. - PubMed
-
- Nashef SAM, Rogues F, Michel P, Gauducheau E, Lemeshow S, Salamon R. Euro Ssg. European system for cardiac operative risk evaluation (euroscore) Eur. J. Cardio-Thorac. Surg. 1999;16:9–13. - PubMed
-
- Ivanov J, Tu JV, Naylor CD. Ready-made, recalibrated, or remodeled? Issues in the use of risk indexes for assessing mortality after coronary artery bypass graft surgery. Circulation. 1999;99:2098–2104. - PubMed
-
- Geissler HJ, Holzl P, Marohl S, Kuhn-Regnier F, Mehlhorn U, Sudkamp M, de Vivie ER. Risk stratification in heart surgery: Comparison of six score systems. Eur. J. Cardio-Thorac. Surg. 2000;17:400–405. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
