

Management of large and giant vestibular schwannomas
- PMID: 22547964
- PMCID: PMC3312131
- DOI: 10.1055/s-0031-1287680
Management of large and giant vestibular schwannomas
Abstract
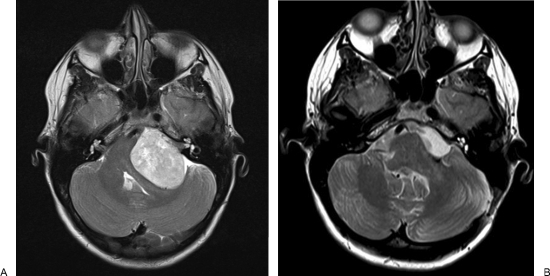
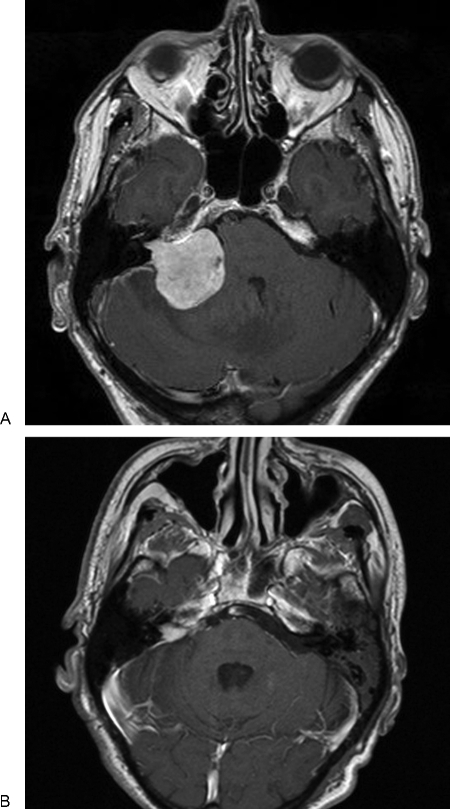
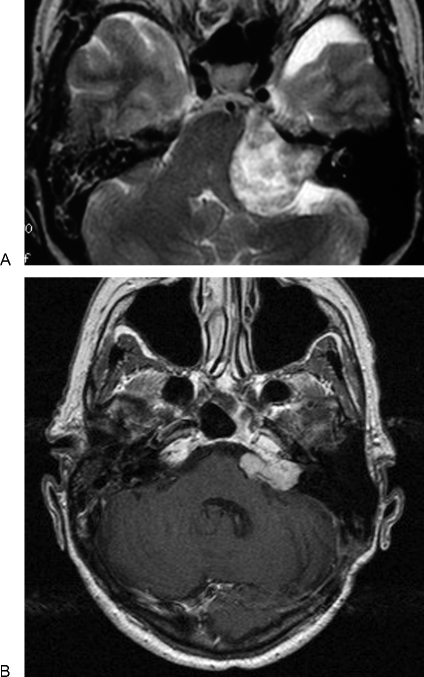
The study was conducted to analyze outcomes following surgical management of large and giant vestibular schwannomas and management options for residual disease. This retrospective case note study includes patients who had undergone microsurgical resection of sporadic, large, or giant vestibular schwannomas from 1986 to 2008. Tumors are classified as large if the largest extracanalicular diameter was 3.5 cm or greater and giant if 4.5 cm or greater. The study included 45 patients (33 large, 12 giant tumors), mean tumor size 4.1 cm. Total excision was achieved in 14 cases (31.1%), near-total in 26 (57.8%), and subtotal in 5 (11.1%). Facial nerve outcome was House-Brackmann Grade I/II in 25 cases (55.6%), III/IV in 16 (35.6%), and V/VI in 4 (8.9%). No recurrence has been detected in those undergoing a complete resection. No residual tumor growth been observed in 15 of 26 who underwent near-total resection (57.7%). Of 11 patients, 10 received further treatment as their residual tumors showed growth. In the subtotal excision group, one patient died, three have demonstrated no growth, and one residual tumor has grown slightly but not required intervention. Optimal management for patients with large or giant vestibular schwannomas has yet to be determined. Management decisions must balance long term function with tumor control.
Keywords: Large vestibular schwannomas; management; residual disease; stereotactic radiotherapy.
Figures
References
-
- Nikolopoulos T P, Fortnum H, O'Donoghue G, Baguley D. Acoustic neuroma growth: a systematic review of the evidence. Otol Neurotol. 2010;31(3):478–485. - PubMed
-
- Verma S, Anthony R, Tsai V, Taplin M, Rutka J. Evaluation of cost effectiveness for conservative and active management strategies for acoustic neuroma. Clin Otolaryngol. 2009;34(5):438–446. - PubMed
-
- Solares C A, Panizza B. Vestibular schwannoma: an understanding of growth should influence management decisions. Otol Neurotol. 2008;29(6):829–834. - PubMed
-
- Mandl E S, Meijer O W, Slotman B J, Vandertop W P, Peerdeman S M. Stereotactic radiation therapy for large vestibular schwannomas. Radiother Oncol. 2010;95(1):94–98. - PubMed
-
- Chung W Y, Pan D H, Lee C C, et al. Large vestibular schwannomas treated by Gamma Knife surgery: long-term outcomes. J Neurosurg. 2010;113(Suppl):112–121. - PubMed
