Temporomandibular disorders. A case-control study
- PMID: 22549687
- PMCID: PMC3482524
- DOI: 10.4317/medoral.18040
Temporomandibular disorders. A case-control study
Abstract
Objective: To compare the risk factors and clinical manifestations of patients with temporomandibular disorders (TMDs) diagnosed according to the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) (axis I) versus an age and gender matched control group.
Study design: A total of 162 patients explored according to the RDC/TMD (mean age 40.6±18.8 years, range 7-90; 11.1% males and 88.9% females) were compared with 119 controls, measuring differences in TMD risk factors (sleep disturbances, stress, psychoactive medication, parafunctions, loss of posterior support, ligament hyperlaxity) and clinical variables (joint sounds, painful muscle and joint palpation, maximum aperture).
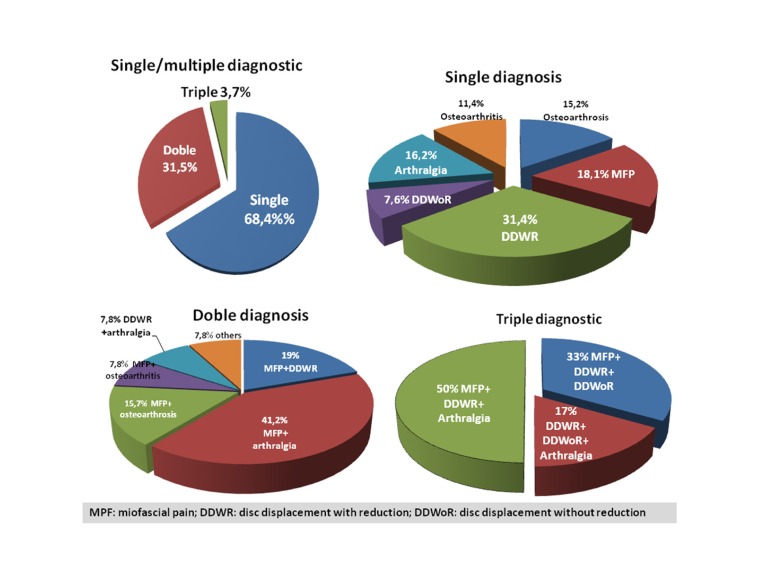
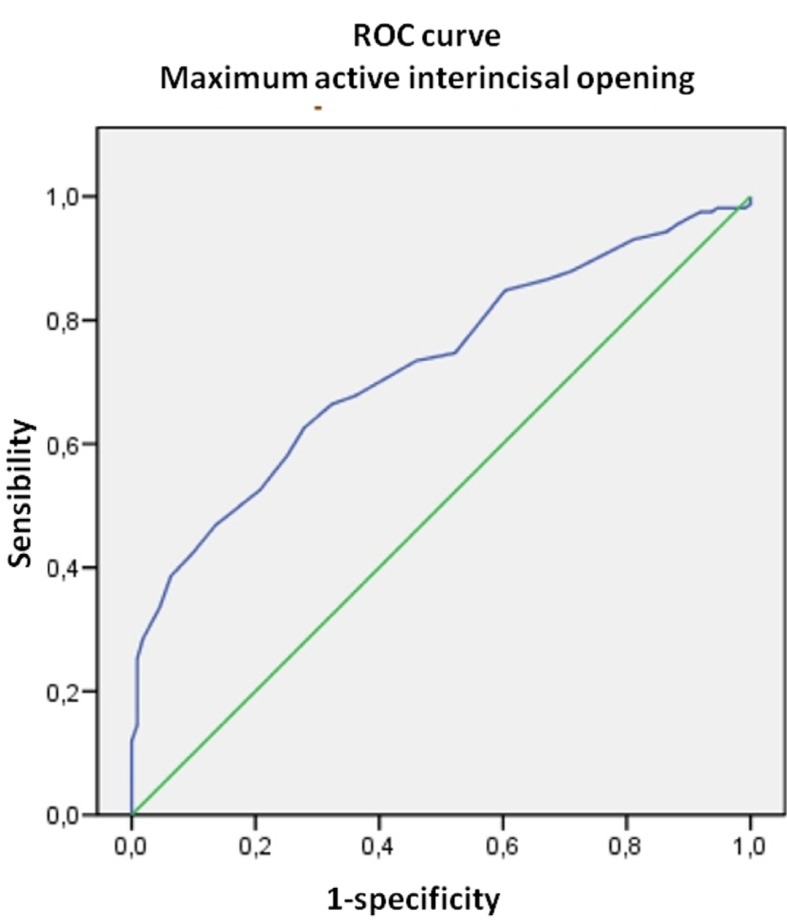
Results: Myofascial pain (MFP) (single or multiple diagnoses) was the most frequent diagnosis (42%). The most common diagnostic combination was MFP plus arthralgia (16.0%). Statistically significant differences were observed in clenching (OR 2.3; 95%CI: 1.4-3.8) and in maximum active aperture (MAA) on comparing the two groups both globally (TMD vs. controls) (patients 36.7±8.6 mm, controls 43.1±5.8 mm; F=45.41, p=0.000) and on comparing according to diagnostic categories. MFP explained most of the observed differences in the risk factors: stress perception (OR=1.98;I.C.:1.01-3.89), psychoactive medication (OR=2.21; I.C.:1.12-4.37), parafunctions (OR=2.14;I.C.:1.12-4.11), and ligament laxity (OR=2.6;I.C.:1.01-6.68). Joint sounds were more frequent in patients with MFP (39.7% vs. 24.0%; χ²=4.66; p=0.03), and painful joint palpation was more common in patients with disc displacement with reduction (DDWR)(15.9% vs. 5.0%; χ²= 5.2; p=0.02) and osteoarthrosis (20.8% vs. 5.0%; χ²=7.0; p=0.008).
Conclusions: There is a high prevalence of signs and symptoms of TMDs in the general population. Significant differences are observed in clenching and MAA between patients and controls considered both globally and for each diagnostic category individually. The analyzed risk factors (except loss of posterior support) show a statistically significant OR for the diagnosis of MFP.
Figures
References
-
- Al-Jundi MA, John MT, Setz JM, Szentpétery A, Kuss O. Meta-analysis of treatment need for temporomandibular disorders in adult nonpatients. J Orofac Pain. 2008;22:97–107. - PubMed
-
- Carlsson GE. Epidemiology and treatment need for temporomandibular disorders. J Orofac Pain. 1999;13:232–7. - PubMed
-
- McMillan AS, Wong MC, Zheng J, Lam CL. Prevalence of orofacial pain and treatment seeking in Hong Kong Chinese. J Orofac Pain. 2006;20:218–25. - PubMed
-
- Dworkin SF, LeResche L. Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord. 1992;6:301–55. - PubMed
-
- List T, Greene CS. Moving forward with the RDC/TMD. J Oral Rehabil. 2010;37:731–3. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical