

Association between treatment with brachytherapy vs whole-breast irradiation and subsequent mastectomy, complications, and survival among older women with invasive breast cancer
- PMID: 22550197
- PMCID: PMC3397792
- DOI: 10.1001/jama.2012.3481
Association between treatment with brachytherapy vs whole-breast irradiation and subsequent mastectomy, complications, and survival among older women with invasive breast cancer
Abstract
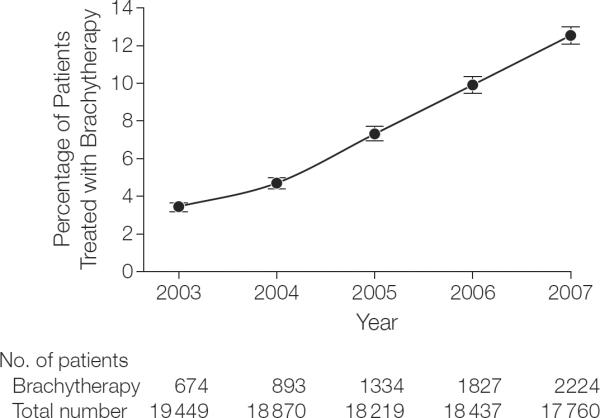
Context: Brachytherapy is a radiation treatment that uses an implanted radioactive source. In recent years, use of breast brachytherapy after lumpectomy for early breast cancer has increased substantially despite a lack of randomized trial data comparing its effectiveness with standard whole-breast irradiation (WBI). Because results of long-term randomized trials will not be reported for years, detailed analysis of clinical outcomes in a nonrandomized setting is warranted.
Objective: To compare the likelihood of breast preservation, complications, and survival for brachytherapy vs WBI among a nationwide cohort of older women with breast cancer with fee-for-service Medicare.
Design: Retrospective population-based cohort study of 92,735 women aged 67 years or older with incident invasive breast cancer, diagnosed between 2003 and 2007 and followed up through 2008. After lumpectomy 6952 patients were treated with brachytherapy vs 85,783 with WBI.
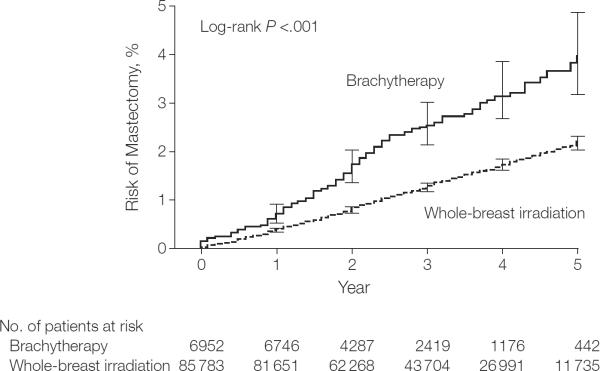
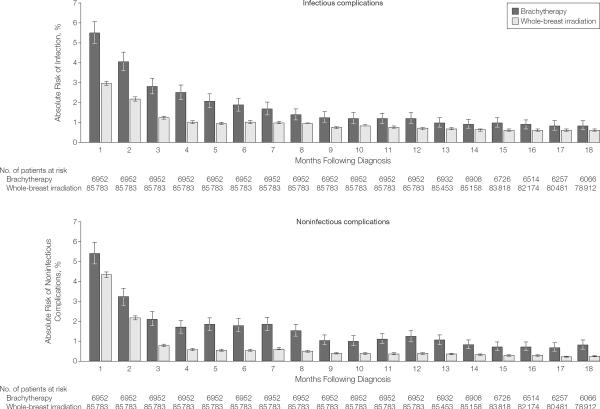
Main outcome measures: Cumulative incidence and adjusted risk of subsequent mastectomy (an indicator of failure to preserve the breast) and death were compared using the log-rank test and proportional hazards models. Odds of postoperative infectious and noninfectious complications within 1 year were compared using the χ(2) test and logistic models. Cumulative incidences of long-term complications were compared using the log-rank test.
Results: Five-year incidence of subsequent mastectomy was higher in women treated with brachytherapy (3.95%; 95% CI, 3.19%-4.88%) vs WBI (2.18%; 95% CI, 2.04%-2.33%; P < .001) and persisted after multivariate adjustment (hazard ratio [HR], 2.19; 95% CI, 1.84-2.61, P < .001). Brachytherapy was associated with more frequent infectious (16.20%; 95% CI, 15.34%-17.08% vs 10.33%; 95% CI, 10.13%-10.53%; P < .001; adjusted odds ratio [OR], 1.76; 1.64-1.88) and noninfectious (16.25%; 95% CI, 15.39%-17.14% vs 9.00%; 95% CI, 8.81%-9.19%; P < .001; adjusted OR, 2.03; 95% CI, 1.89-2.17) postoperative complications; and higher 5-year incidence of breast pain (14.55%, 95% CI, 13.39%-15.80% vs 11.92%; 95% CI, 11.63%-12.21%), fat necrosis (8.26%; 95% CI, 7.27-9.38 vs 4.05%; 95% CI, 3.87%-4.24%), and rib fracture (4.53%; 95% CI, 3.63%-5.64% vs 3.62%; 95% CI, 3.44%-3.82%; P ≤ .01 for all). Five-year overall survival was 87.66% (95% CI, 85.94%-89.18%) in patients treated with brachytherapy vs 87.04% (95% CI, 86.69%-87.39%) in patients treated with WBI (adjusted HR, 0.94; 95% CI, 0.84-1.05; P = .26).
Conclusion: In a cohort of older women with breast cancer, treatment with brachytherapy compared with WBI was associated worse with long-term breast preservation and increased complications but no difference in survival.
Figures
Comment in
-
Breast cancer: Whole is better than the part.Nat Rev Clin Oncol. 2012 May 29;9(7):370. doi: 10.1038/nrclinonc.2012.97. Nat Rev Clin Oncol. 2012. PMID: 22641366 No abstract available.
-
Brachytherapy vs whole-breast irradiation for breast cancer.JAMA. 2012 Aug 8;308(6):567; author reply 567-8. doi: 10.1001/jama.2012.8486. JAMA. 2012. PMID: 22871864 No abstract available.
-
[Evaluation of (balloon) brachytherapy for partial breast irradiation in breast cancer based on current meta-analyses].Strahlenther Onkol. 2013 Oct;189(10):899-901. doi: 10.1007/s00066-013-0425-z. Strahlenther Onkol. 2013. PMID: 23963208 German. No abstract available.
References
-
- Smith BD, Arthur DW, Buchholz TA, et al. Accelerated partial breast irradiation consensus statement from the American Society for Radiation Oncology (ASTRO) Int J Radiat Oncol Biol Phys. 2009;74(4):987–1001. - PubMed
-
- Smith BD, Arthur DW, Buchholz TA, et al. Accelerated partial breast irradiation consensus statement from the American Society for Radiation Oncology (ASTRO) J Am Coll Surg. 2009;209(2):269–277. - PubMed
-
- Smith GL, Xu Y, Buchholz TA, et al. Brachytherapy for accelerated partial-breast irradiation. J Clin Oncol. 2011;29(2):157–165. - PubMed
-
- Abbott AM, Habermann EB, Tuttle TM. Trends in the use of implantable accelerated partial breast irradiation therapy for early stage breast cancer in the United States. Cancer. 2011;117(15):3305–3310. - PubMed
-
- Hattangadi JA, Taback N, Neville BA, Harris JR, Punglia RS. Accelerated partial breast irradiation using brachytherapy for breast cancer. J Natl Cancer Inst. 2012;104(1):29–41. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
