

Pendelluft in chronic obstructive lung disease measured with lung sounds
- PMID: 22550582
- PMCID: PMC3324918
- DOI: 10.1155/2012/139395
Pendelluft in chronic obstructive lung disease measured with lung sounds
Abstract
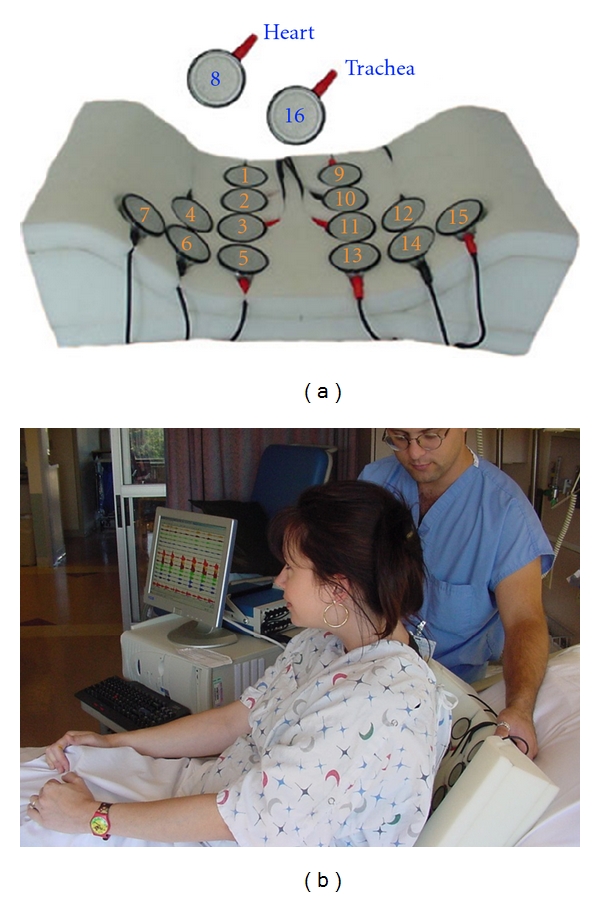
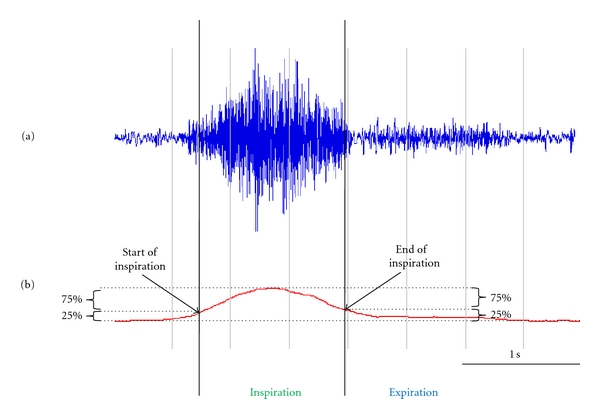
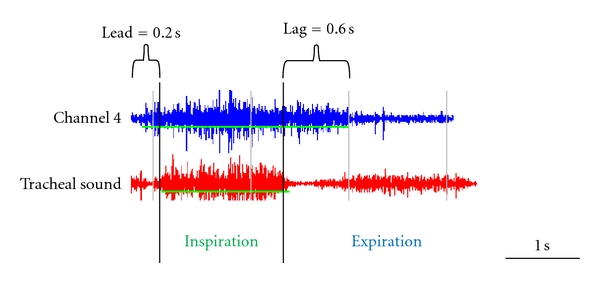
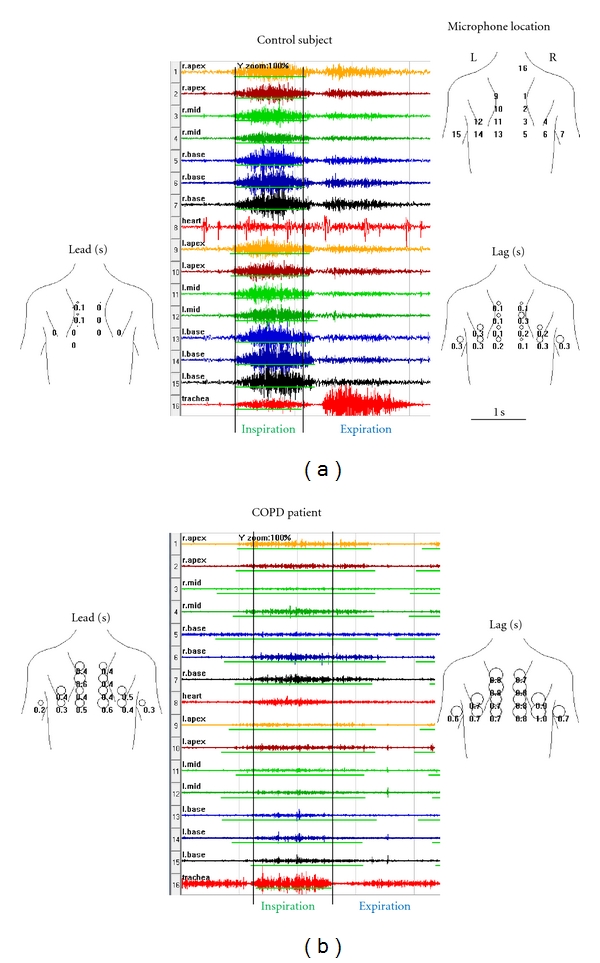
Objective. The phenomenon of pendelluft was described over five decades ago. In patients with regional variations in resistance and elastance, gas moves at the beginning of inspiration out of some alveoli into others. Gas moves in the opposite direction at the end of inspiration. The objective of this study was to apply the method of lung sounds mapping, which is known to provide regional information about gas flow, to study pendelluft in COPD patients. Methods. A 16-channel lung sound analyzer was used to collect sounds from patients with COPD (n = 90) and age-matched normals (n = 90). Pendelluft at the beginning of inspiration is expected to result in vesicular sounds leading the tracheal sound by a few milliseconds. Pendelluft at the end of inspiration is expected to result in vesicular sounds lagging the tracheal sound. These lead and lag times were calculated for the 14 chest wall sites. Results. The lead time was significantly longer in COPD patients: 123 ± 107 ms versus 48 ± 59 ms in controls (P < 0.0001). The lag time was also significantly longer in COPD patients: 269 ± 249 ms in COPD patients versus 147 ± 124 ms in controls (P < 0.0001). When normalized by the duration of the inspiration at the trachea, the lead was 14 ± 13% for COPD versus 4 ± 5% for controls (P < 0.0001). The lag was 28 ± 25% for COPD versus 13 ± 12% for controls (P < 0.0001). Both lead and lag correlated moderately with the GOLD stage (correlation coefficient 0.43). Conclusion. Increased lead and lag times in COPD patients are consistent with the phenomenon of pendelluft as has been observed by other methods.
Figures
References
-
- Otis AB, Mckerrow CB, Bartlett RA, et al. Mechanical factors in distribution of pulmonary ventilation. Journal of Applied Physiology. 1956;8(4):427–443. - PubMed
-
- Hogg JC. Pathophysiology of airflow limitation in chronic obstructive pulmonary disease. Lancet. 2004;364(9435):709–721. - PubMed
-
- Nairn JR, Turner-Warwick M. Breath sounds in emphysema. British Journal of Diseases of the Chest. 1969;63(1):29–37. - PubMed
-
- LeBlanc P, Macklem PT, Ross WRD. Breath sounds and distribution of pulmonary ventilation. American Review of Respiratory Disease. 1970;102(1):10–16. - PubMed
LinkOut - more resources
Full Text Sources
