

Warfarin and aspirin in patients with heart failure and sinus rhythm
- PMID: 22551105
- PMCID: PMC3723382
- DOI: 10.1056/NEJMoa1202299
Warfarin and aspirin in patients with heart failure and sinus rhythm
Abstract
Background: It is unknown whether warfarin or aspirin therapy is superior for patients with heart failure who are in sinus rhythm.
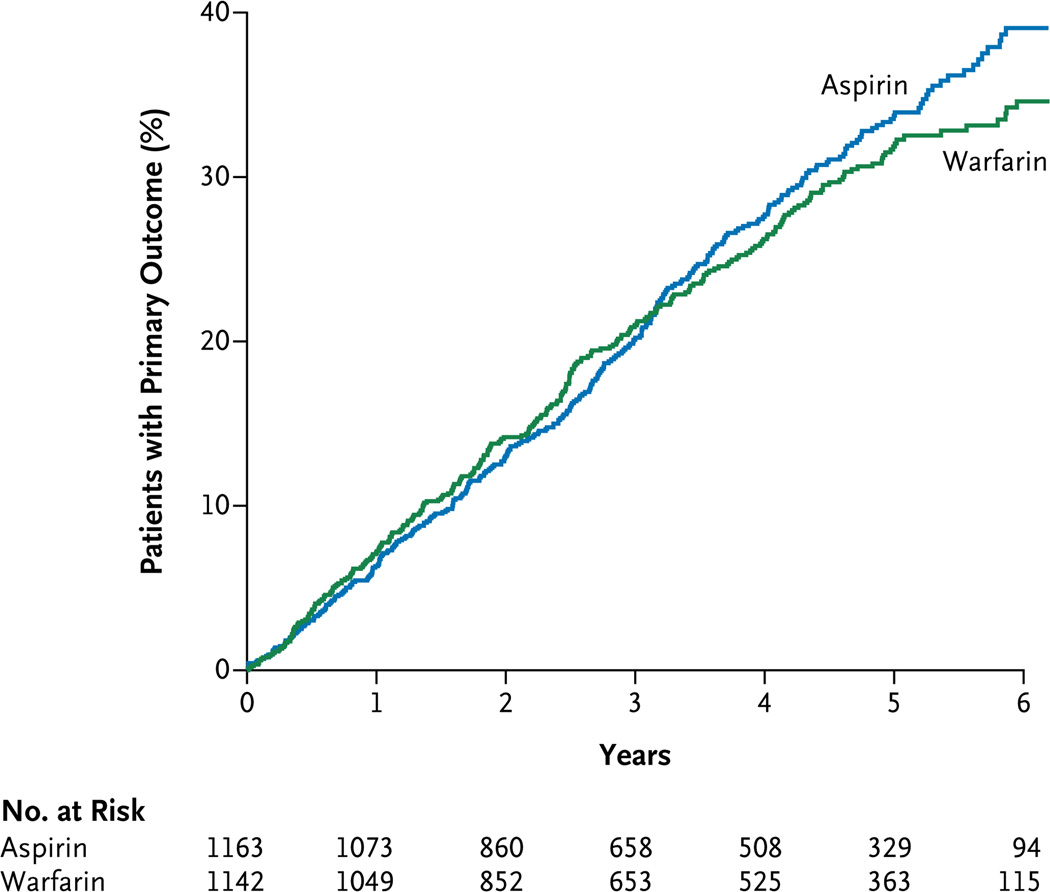
Methods: We designed this trial to determine whether warfarin (with a target international normalized ratio of 2.0 to 3.5) or aspirin (at a dose of 325 mg per day) is a better treatment for patients in sinus rhythm who have a reduced left ventricular ejection fraction (LVEF). We followed 2305 patients for up to 6 years (mean [±SD], 3.5±1.8). The primary outcome was the time to the first event in a composite end point of ischemic stroke, intracerebral hemorrhage, or death from any cause.
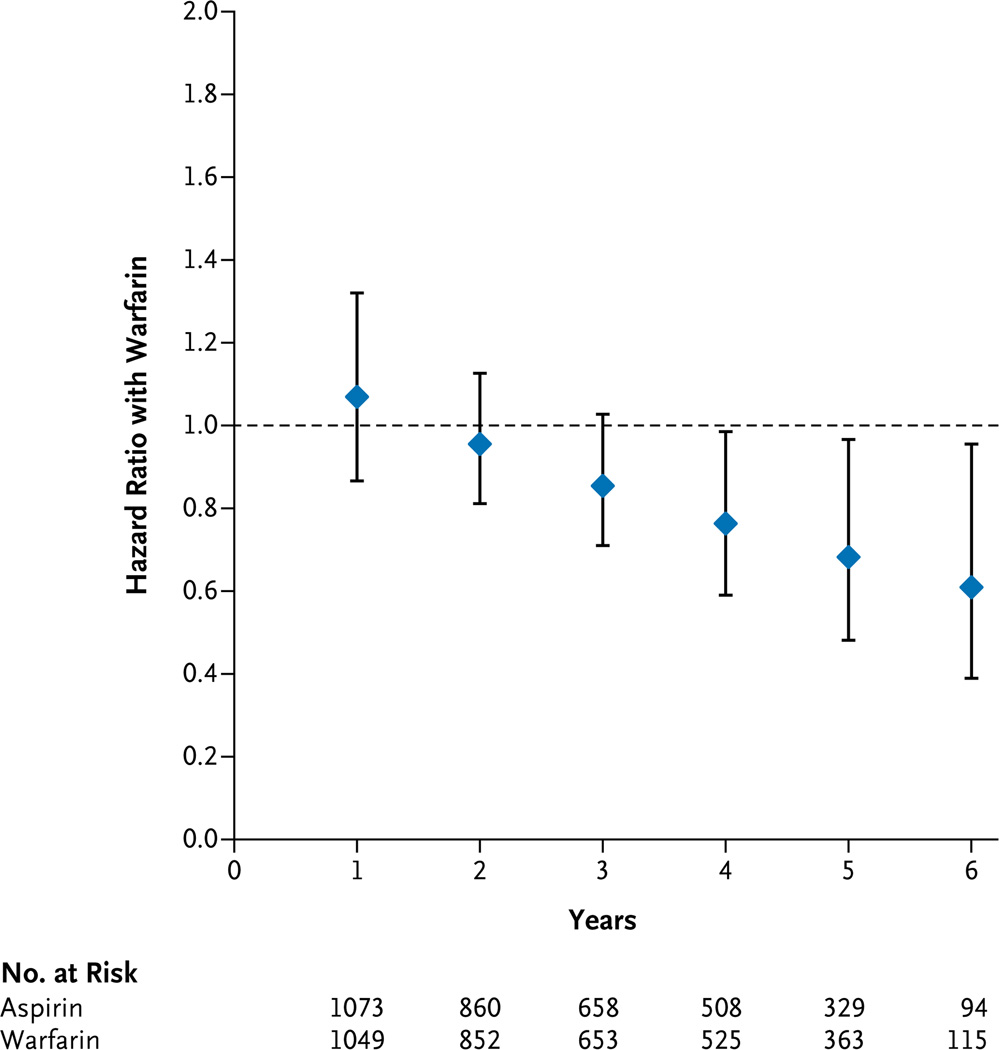
Results: The rates of the primary outcome were 7.47 events per 100 patient-years in the warfarin group and 7.93 in the aspirin group (hazard ratio with warfarin, 0.93; 95% confidence interval [CI], 0.79 to 1.10; P=0.40). Thus, there was no significant overall difference between the two treatments. In a time-varying analysis, the hazard ratio changed over time, slightly favoring warfarin over aspirin by the fourth year of follow-up, but this finding was only marginally significant (P=0.046). Warfarin, as compared with aspirin, was associated with a significant reduction in the rate of ischemic stroke throughout the follow-up period (0.72 events per 100 patient-years vs. 1.36 per 100 patient-years; hazard ratio, 0.52; 95% CI, 0.33 to 0.82; P=0.005). The rate of major hemorrhage was 1.78 events per 100 patient-years in the warfarin group as compared with 0.87 in the aspirin group (P<0.001). The rates of intracerebral and intracranial hemorrhage did not differ significantly between the two treatment groups (0.27 events per 100 patient-years with warfarin and 0.22 with aspirin, P=0.82).
Conclusions: Among patients with reduced LVEF who were in sinus rhythm, there was no significant overall difference in the primary outcome between treatment with warfarin and treatment with aspirin. A reduced risk of ischemic stroke with warfarin was offset by an increased risk of major hemorrhage. The choice between warfarin and aspirin should be individualized. (Funded by the National Institute of Neurological Disorders and Stroke; WARCEF ClinicalTrials.gov number, NCT00041938.).
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Warfarin in heart failure.N Engl J Med. 2012 May 17;366(20):1936-8. doi: 10.1056/NEJMe1202504. Epub 2012 May 2. N Engl J Med. 2012. PMID: 22551103 No abstract available.
-
Anticoagulation therapies: Warfarin vs aspirin in HF.Nat Rev Cardiol. 2012 May 22;9(7):372. doi: 10.1038/nrcardio.2012.77. Nat Rev Cardiol. 2012. PMID: 22614619 No abstract available.
-
ACP Journal Club: warfarin and aspirin did not differ for death or stroke in heart failure and sinus rhythm.Ann Intern Med. 2012 Aug 21;157(4):JC2-7. doi: 10.7326/0003-4819-157-4-201208210-02007. Ann Intern Med. 2012. PMID: 22910961 No abstract available.
-
Warfarin versus aspirin in heart failure and sinus rhythm.N Engl J Med. 2012 Aug 23;367(8):771; author reply 772. doi: 10.1056/NEJMc1207385. N Engl J Med. 2012. PMID: 22913690 No abstract available.
-
Warfarin versus aspirin in heart failure and sinus rhythm.N Engl J Med. 2012 Aug 23;367(8):771-2; author reply 772. doi: 10.1056/NEJMc1207385. N Engl J Med. 2012. PMID: 22913691 No abstract available.
-
Thromboprophylaxis in heart failure patients with sinus rhythm: aspirin and warfarin lead to similar cardiovascular outcomes.Evid Based Med. 2013 Apr;18(2):69-70. doi: 10.1136/eb-2012-100877. Epub 2012 Aug 23. Evid Based Med. 2013. PMID: 22918068 No abstract available.
-
[Journal club].Z Gerontol Geriatr. 2012 Oct;45(7):673-4. doi: 10.1007/s00391-012-0378-3. Z Gerontol Geriatr. 2012. PMID: 23052284 German. No abstract available.
-
Update in general internal medicine: evidence published in 2012.Ann Intern Med. 2013 Apr 16;158(8):615-9. doi: 10.7326/0003-4819-158-8-201304160-00101. Ann Intern Med. 2013. PMID: 23579948 No abstract available.
References
-
- Kalaria VG, Passannante MR, Shah T, Modi K, Weisse AB. Effect of mitral regurgitation on left ventricular thrombus formation in dilated cardiomyopathy. Am Heart J. 1998;135:215–220. - PubMed
-
- Lip GYH, Gibbs CR. Does heart failure confer a hypercoagulable state? Virchow’s triad revisited. J Am Coll Cardiol. 1999;33:1424–1426. - PubMed
-
- Uretsky BF, Thygesen K, Armstrong PW, et al. Acute coronary findings at autopsy in heart failure patients with sudden death: results from the Assessment of Treatment With Lisinopril and Survival (ATLAS) trial. Circulation. 2000;102:611–616. - PubMed
-
- Freudenberger RS, Halperin JL. Should we use anticoagulation for patients with chronic heart failure? Nat Clin Pract Cardiovasc Med. 2006;3:580–581. - PubMed
-
- Ezekowitz M. Antithrombotics for leftventricular impairment? Lancet. 1998;351:1904. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical