

Inadequate dietary intake in patients with thalassemia
- PMID: 22551675
- PMCID: PMC3419338
- DOI: 10.1016/j.jand.2012.01.017
Inadequate dietary intake in patients with thalassemia
Abstract
Background: Patients with thalassemia have low circulating levels of many nutrients, but the contribution of dietary intake has not been assessed.
Objective: Our objective was to assess dietary intake in a large contemporary sample of subjects with thalassemia.
Design: A prospective, longitudinal cohort study using a validated food frequency questionnaire was conducted.
Participants/setting: Two hundred and twenty-one subjects (19.7±11.3 years, 106 were female) were categorized into the following age groups: young children (3 to 7.9 years), older children/adolescents (8 to 18.9 years), and adults (19 years or older); 78.8% had β-thalassemia and 90% were chronically transfused. This study took place at 10 hematology outpatient clinics in the United States and Canada.
Main outcome measures: We conducted a comparison of intake with US Dietary Reference Intakes and correlated dietary intake of vitamin D with serum 25-OH vitamin D and dietary iron with total body iron stores.
Statistical analyses performed: Intake was defined as inadequate if it was less than the estimated average requirement. χ(2), Fisher's exact, and Student's t test were used to compare intake between age categories and logistic regression analysis to test the relationship between intake and outcomes, controlling for age, sex, and race.
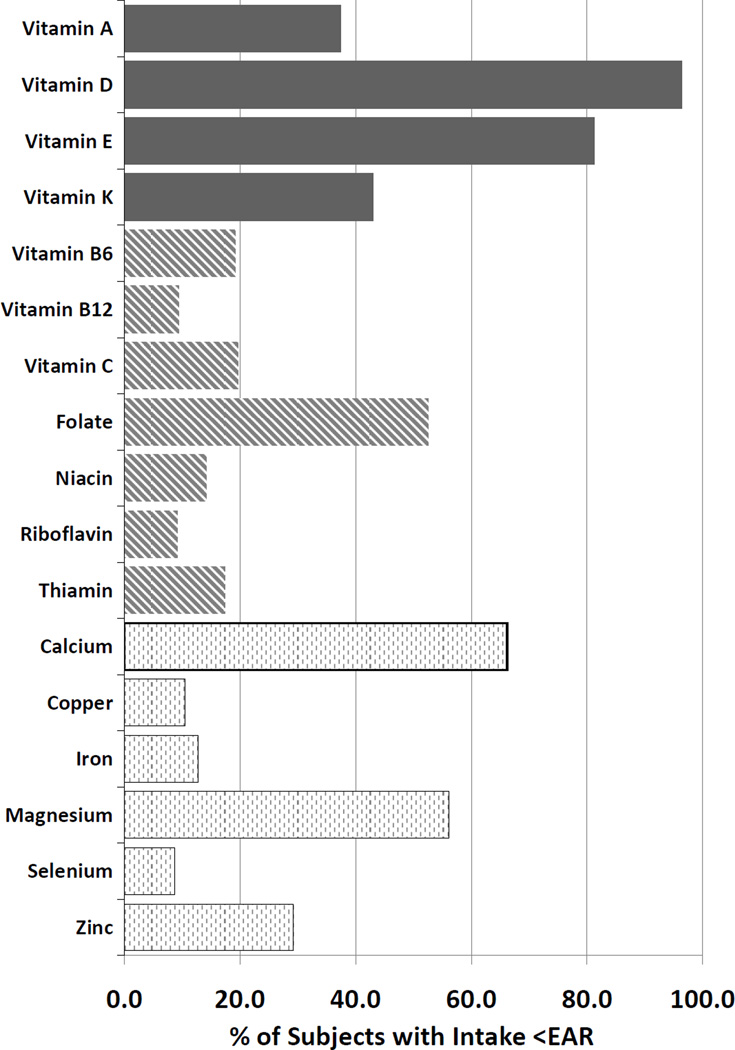
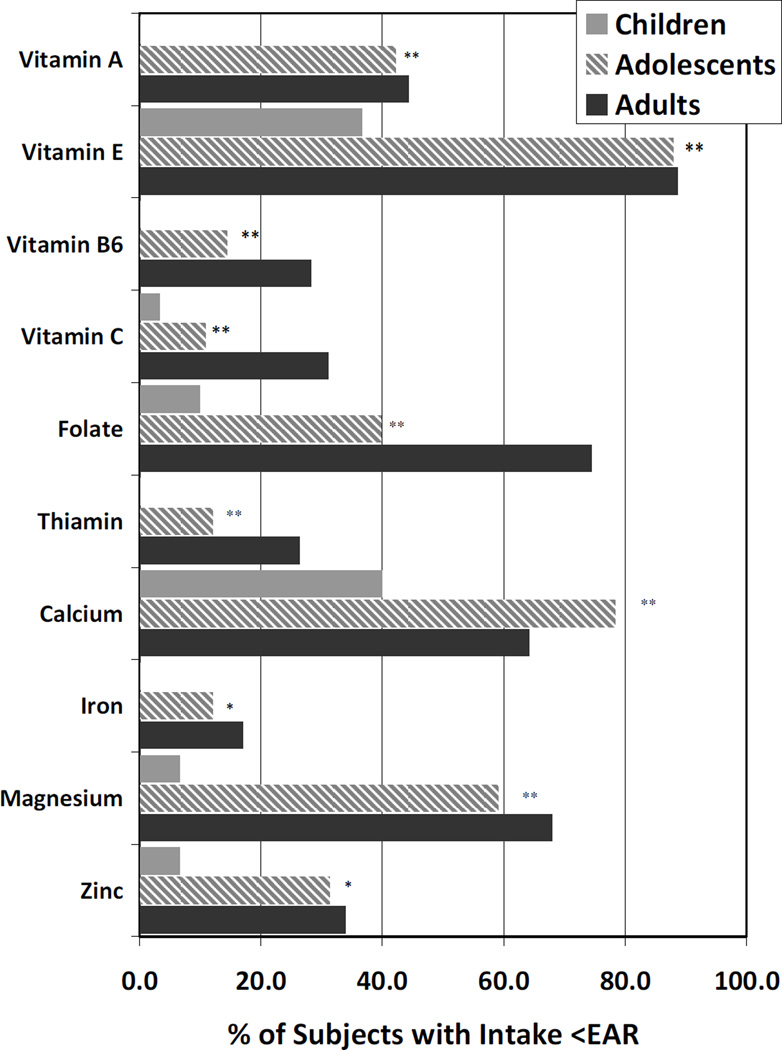
Results: More than 30% of subjects consumed inadequate levels of vitamin A, D, E, K, folate, calcium, and magnesium. The only nutrients for which >90% of subjects consumed adequate amounts were riboflavin, vitamin B-12, and selenium. Dietary inadequacy increased with increasing age group (P<0.01) for vitamins A, C, E, B-6, folate, thiamin, calcium, magnesium, and zinc. More than half of the sample took additional supplements of calcium and vitamin D, although circulating levels of 25-OH vitamin D remained insufficient in 61% of subjects. Dietary iron intake was not related to total body iron stores.
Conclusions: Subjects with thalassemia have reduced intake of many key nutrients. These preliminary findings of dietary inadequacy are concerning and support the need for nutritional monitoring to determine which subjects are at greatest risk for nutritional deficiency. Future research should focus on the effect of dietary quality and nutritional status on health outcomes in thalassemia.
Copyright © 2012 Academy of Nutrition and Dietetics. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Vichinsky EP. Changing patterns of thalassemia worldwide. Ann NY Acad Sci. 2005;1054:18–24. - PubMed
-
- Cunningham MJ, Macklin EA, Neufeld EJ, Cohen AR. Complications of B-thalassemia major in North America. Blood. 2004;104(1):34–39. - PubMed
-
- Vichinsky EP, Macklin EA, Waye JS, Lorey F, Olivieri NF. Changes in the epidemiology of thalassemia in North America: a new minority disease. Pediatrics. 2005;116(6):e818–e825. - PubMed
-
- Zurlo MG, De Stefano P, Borgna-Pignatti C, et al. Survival and causes of death in thalassaemia major. Lancet. 1989;2(8653):27–30. - PubMed
-
- Fung EB, Harmatz P, Milet M, et al. Morbidity and mortality in chronically transfused subjects with thalassemia or sickle cell disease: a report from the multicenter study of iron overload. Am J Hematol. 2007;82(4):255–265. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U-01RR025758/RR/NCRR NIH HHS/United States
- U01-HL65238/HL/NHLBI NIH HHS/United States
- U01 HL065260/HL/NHLBI NIH HHS/United States
- UL1-RR024131/RR/NCRR NIH HHS/United States
- U01-HL72291/HL/NHLBI NIH HHS/United States
- U01 HL065239/HL/NHLBI NIH HHS/United States
- UL1-RR024134/RR/NCRR NIH HHS/United States
- UL1-RR024996/RR/NCRR NIH HHS/United States
- U01-HL65233/HL/NHLBI NIH HHS/United States
- U01-HL65244/HL/NHLBI NIH HHS/United States
- U01-HL65239/HL/NHLBI NIH HHS/United States
- UL1 RR025758/RR/NCRR NIH HHS/United States
- U01-HL65232/HL/NHLBI NIH HHS/United States
