

Myasthenia gravis and neuromyelitis optica spectrum disorder: a multicenter study of 16 patients
- PMID: 22551731
- PMCID: PMC3348852
- DOI: 10.1212/WNL.0b013e31825644ff
Myasthenia gravis and neuromyelitis optica spectrum disorder: a multicenter study of 16 patients
Abstract
Objective: To describe 16 patients with a coincidence of 2 rare diseases: aquaporin-4 antibody (AQP4-Ab)-mediated neuromyelitis optica spectrum disorder (AQP4-NMOSD) and acetylcholine receptor antibody (AChR-Ab)-mediated myasthenia gravis (AChR-MG).
Methods: The clinical details and antibody results of 16 patients with AChR-MG and AQP4-NMOSD were analyzed retrospectively.
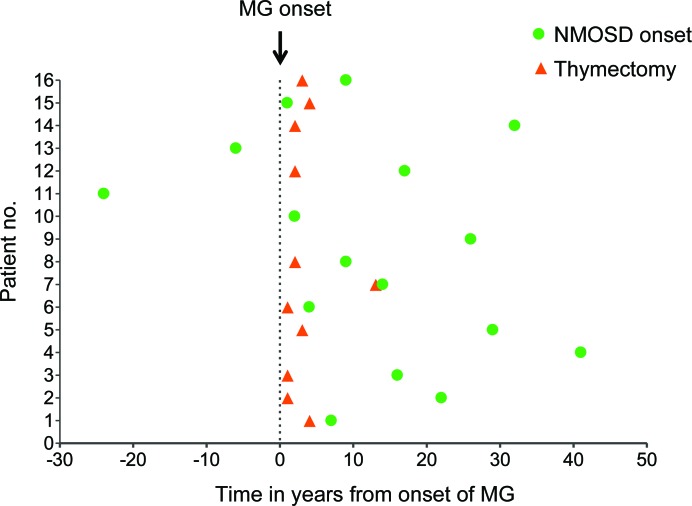
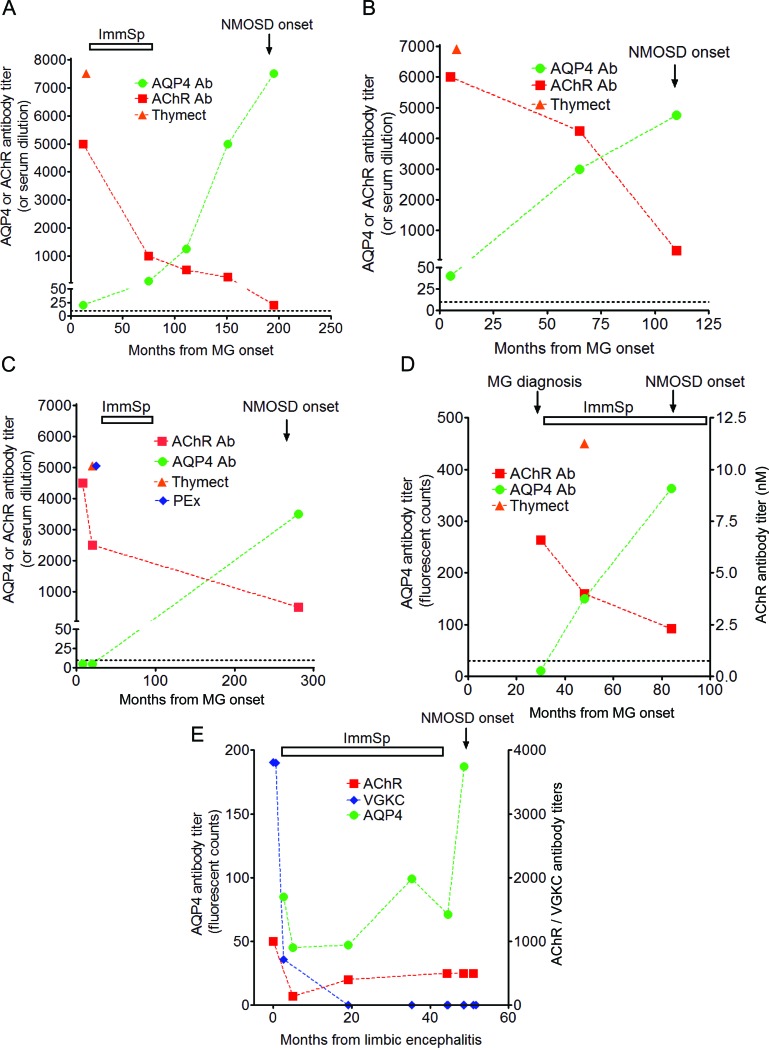
Results: All had early-onset AChR-MG, the majority with mild generalized disease, and a high proportion achieved remission. Fifteen were female; 11 were Caucasian. In 14/16, the MG preceded NMOSD (median interval: 16 years) and 11 of these had had a thymectomy although 1 only after NMOSD onset. In 4/5 patients tested, AQP4-Abs were detectable between 4 and 16 years prior to disease onset, including 2 patients with detectable AQP4-Abs prior to thymectomy. AChR-Abs decreased and the AQP4-Ab levels increased over time in concordance with the relevant disease. AChR-Abs were detectable at NMOSD onset in the one sample available from 1 of the 2 patients with NMOSD before MG.
Conclusions: Although both conditions are rare, the association of MG and NMOSD occurs much more frequently than by chance and the MG appears to follow a benign course. AChR-Abs or AQP4-Abs may be present years before onset of the relevant disease and the antibody titers against AQP4 and AChR tend to change in opposite directions. Although most cases had MG prior to NMOSD onset, and had undergone thymectomy, NMOSD can occur first and in patients who have not had their thymus removed.
Figures
References
-
- Wingerchuk DM, Hogancamp WF, O'Brien PC, Weinshenker BG. The clinical course of neuromyelitis optica (Devic's syndrome). Neurology 1999; 53: 1107– 1114 - PubMed
-
- Waters P, Jarius S, Littleton E, et al. Aquaporin-4 antibodies in neuromyelitis optica and longitudinally extensive transverse myelitis. Arch Neurol 2008; 65: 913– 919 - PubMed
-
- Lennon VA, Wingerchuk DM, Kryzer TJ, et al. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet 2004; 364: 2106– 2112 - PubMed
-
- Wingerchuk DM, Lennon VA, Pittock SJ, Lucchinetti CF, Weinshenker BG. Revised diagnostic criteria for neuromyelitis optica. Neurology 2006; 66: 1485– 1489 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases