

Accuracy of in vivo multimodal optical imaging for detection of oral neoplasia
- PMID: 22551901
- PMCID: PMC3560936
- DOI: 10.1158/1940-6207.CAPR-11-0555
Accuracy of in vivo multimodal optical imaging for detection of oral neoplasia
Abstract
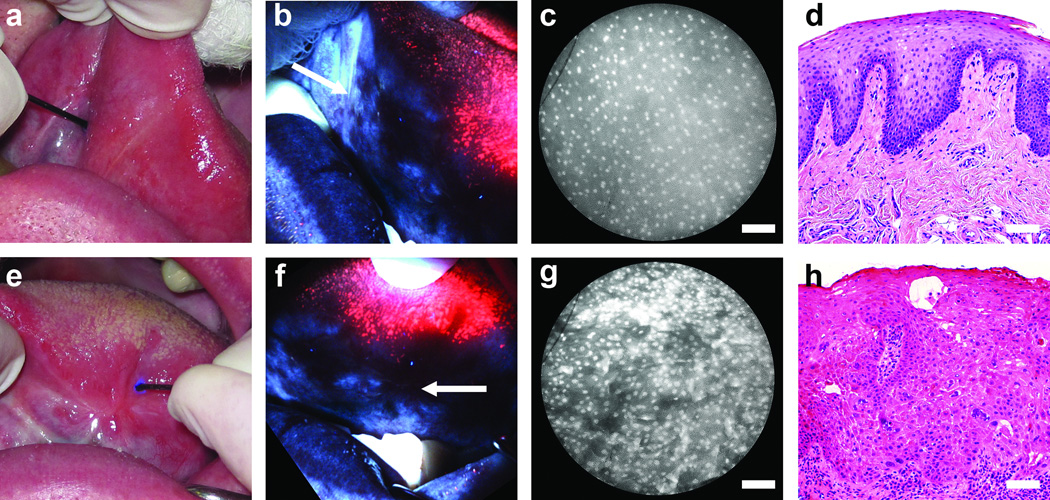
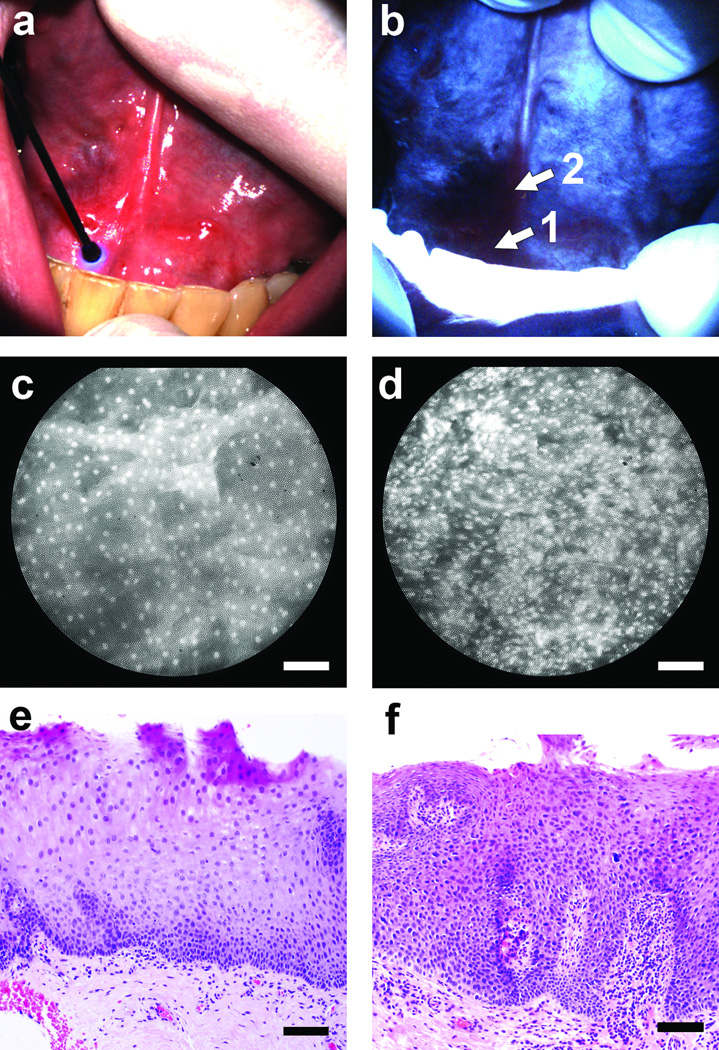
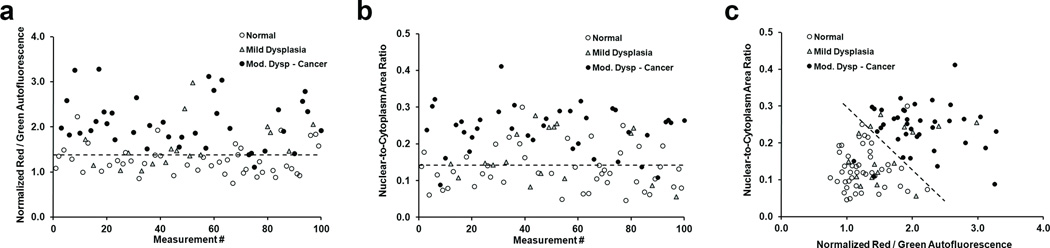
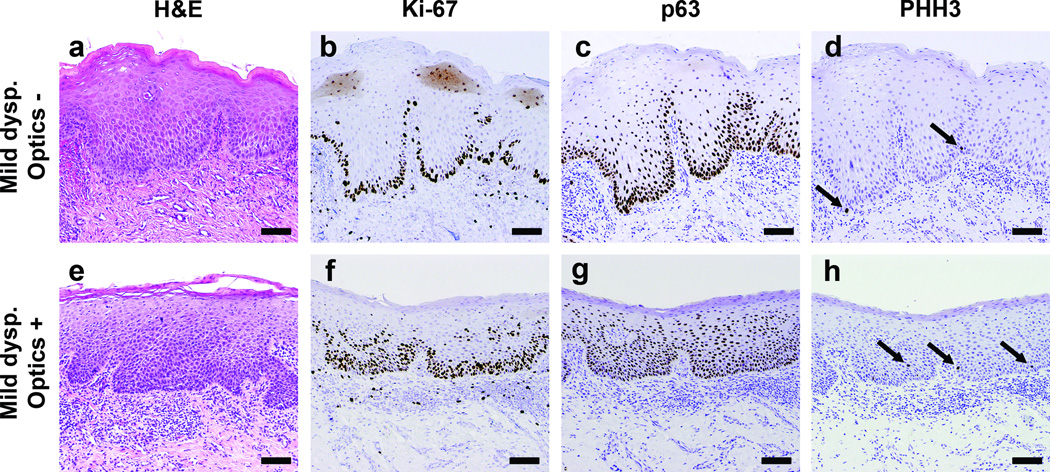
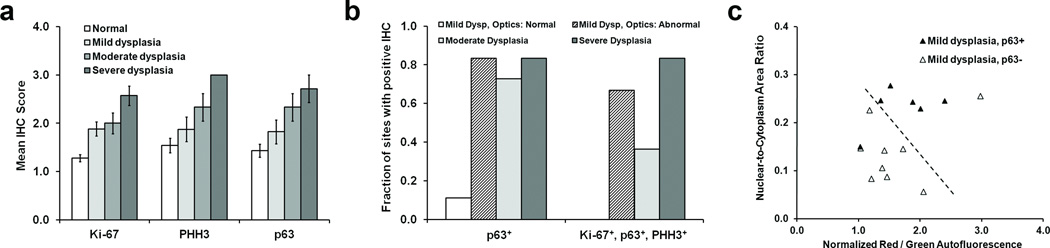
If detected early, oral cancer is eminently curable. However, survival rates for oral cancer patients remain low, largely due to late-stage diagnosis and subsequent difficulty of treatment. To improve clinicians' ability to detect early disease and to treat advanced cancers, we developed a multimodal optical imaging system (MMIS) to evaluate tissue in situ, at macroscopic and microscopic scales. The MMIS was used to measure 100 anatomic sites in 30 patients, correctly classifying 98% of pathologically confirmed normal tissue sites, and 95% of sites graded as moderate dysplasia, severe dysplasia, or cancer. When used alone, MMIS classification accuracy was 35% for sites determined by pathology as mild dysplasia. However, MMIS measurements correlated with expression of candidate molecular markers in 87% of sites with mild dysplasia. These findings support the ability of noninvasive multimodal optical imaging to accurately identify neoplastic tissue and premalignant lesions. This in turn may have considerable impact on detection and treatment of patients with oral cancer and other epithelial malignancies.
©2012 AACR.
Conflict of interest statement
Potential conflict(s) of interest / Disclosure:
Dr. Richards-Kortum serves as an unpaid scientific advisor to Remicalm LLC, holds patents related to optical diagnostic technologies that have been licensed to Remicalm LLC, and holds minority ownership in Remicalm LLC. Dr. Gillenwater has a minority equity interest in Onconome, Inc., and serves as an unpaid scientific advisor to Remicalm LLC. Dr. Schwarz holds a patent related to optical diagnostic technologies that has been licensed to Remicalm LLC.
Figures
References
-
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 10. Lyon, France: International Agency for Research on Cancer; 2010. GLOBOCAN 2008 v1.2.
-
- Chen AY, Myers JN. Cancer of the oral cavity. Dis Mon. 2001;47:275–361. - PubMed
-
- Thomson PJ. Field change and oral cancer: new evidence for widespread carcinogenesis? Int J Oral Maxillofac Surg. 2002;31:262–266. - PubMed
-
- De Veld DC, Witjes MJ, Sterenborg HJ, Roodenburg JL. The status of in vivo autofluorescence spectroscopy and imaging for oral oncology. Oral Oncol. 2005;41:117–131. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
