

Limiting variety in non-nutrient-dense, energy-dense foods during a lifestyle intervention: a randomized controlled trial
- PMID: 22552025
- PMCID: PMC3349452
- DOI: 10.3945/ajcn.111.031153
Limiting variety in non-nutrient-dense, energy-dense foods during a lifestyle intervention: a randomized controlled trial
Abstract
Background: Dietary variety is a factor that influences consumption but has received little attention in obesity treatment.
Objective: This study examined the effect of limiting the variety of different non-nutrient-dense, energy-dense foods (NND-EDFs) (i.e., chips, ice cream, cookies) on dietary intake and weight loss during an 18-mo lifestyle intervention.
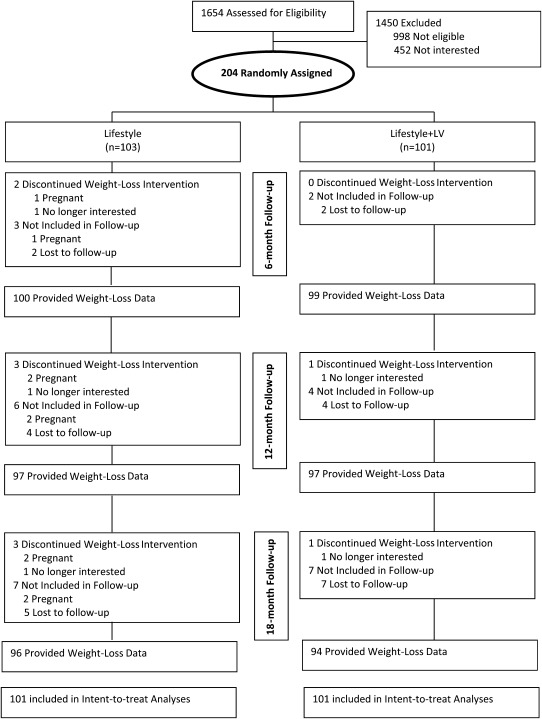
Design: Two hundred two adults aged 51.3 ± 9.5 y with a BMI (in kg/m2) of 34.9 ± 4.3 (57.8% women, 92.2% white) were randomly assigned to 1 of 2 interventions: Lifestyle (1200-1500 kcal/d, ≤30% of energy as fat; n = 101) or Lifestyle + limited variety (LV) (limit variety of NND-EDFs, i.e., 2 choices; n = 101). Both interventions involved 48 group sessions. Dietary intake, NND-EDF hedonics, NND-EDF variety in the home, and weight were assessed at 0, 6, 12, and 18 mo.
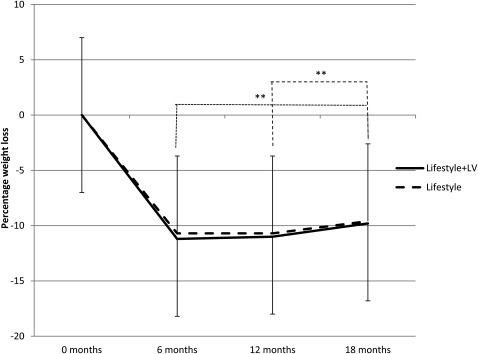
Results: Intent-to-treat analyses showed that the Lifestyle+LV group consumed less variety (P < 0.01) and energy daily (P < 0.05) from NND-EDFs than did the Lifestyle group at 6, 12, and 18 mo. The Lifestyle+LV group consumed less total energy daily (P < 0.05) at 6 mo than did the Lifestyle group. The Lifestyle+LV group reported less (P < 0.05) NND-EDF variety in the home at 6 and 18 mo than did the Lifestyle group. The hedonics of one chosen NND-EDF decreased more (P < 0.05) in the Lifestyle+LV group. Despite these effects, no difference in percentage weight loss occurred at 18 mo (Lifestyle+LV: -9.9 ± 7.6%; Lifestyle: -9.6 ± 9.2%).
Conclusions: Limitations in dietary variety decreased intakes in the targeted area but did not affect weight loss. Limiting variety in more areas may be needed to improve weight loss and weight-loss maintenance. This trial was registered at clinicaltrials.gov as NCT01096719.
Figures


References
-
- Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999-2004. JAMA 2006;295:1549–55 - PubMed
-
- Harris MI, Flegal KM, Cowie CC, Eberhardt MS, Goldstein DE, Little RR, Hsiao-Mei W, Byrd-Holt DD. Prevalence of diabetes, impaired fasting glucose, and impaired glucose tolerance in U.S. adults. The Third National Health and Nutrition Examination Survey, 1988–1994. Diabetes Care 1998;21:518–24 - PubMed
-
- National Heart, Lung, and Blood Institute Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: the evidence report. Obes Res 1998;6:51S–209S - PubMed
-
- Anderson JW, Konz EC. Obesity and disease management: effect of weight loss on comorbid conditions. Obes Res 2001;9:326S–34S - PubMed
