

Molecular and culture-based assessment of the microbial diversity of diabetic chronic foot wounds and contralateral skin sites
- PMID: 22553231
- PMCID: PMC3405613
- DOI: 10.1128/JCM.06599-11
Molecular and culture-based assessment of the microbial diversity of diabetic chronic foot wounds and contralateral skin sites
Abstract
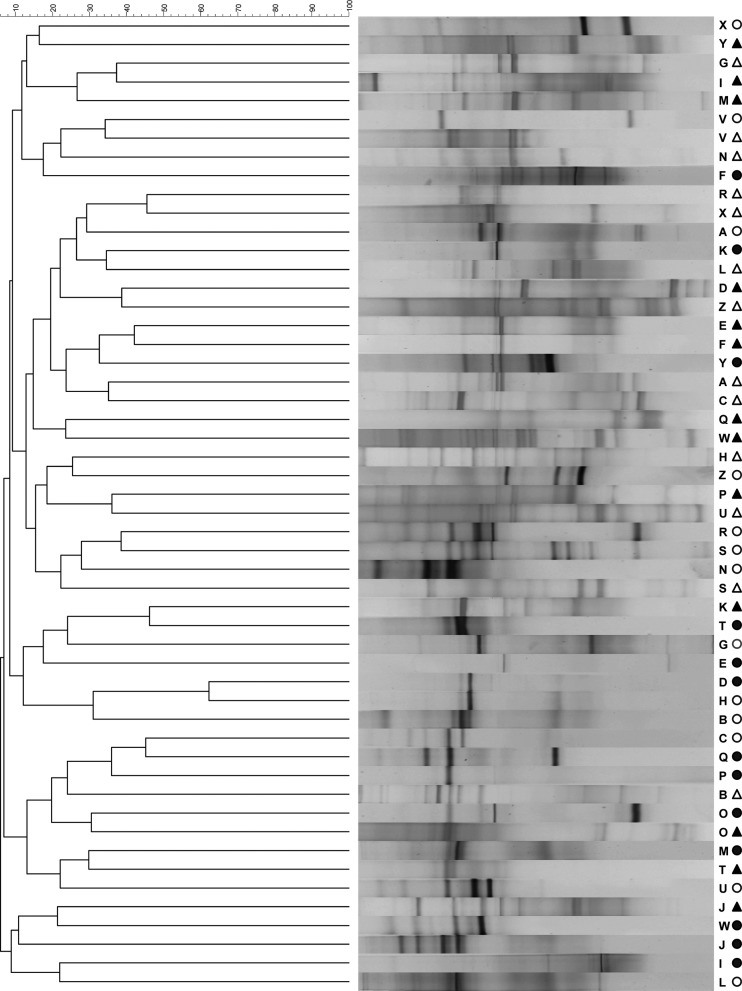
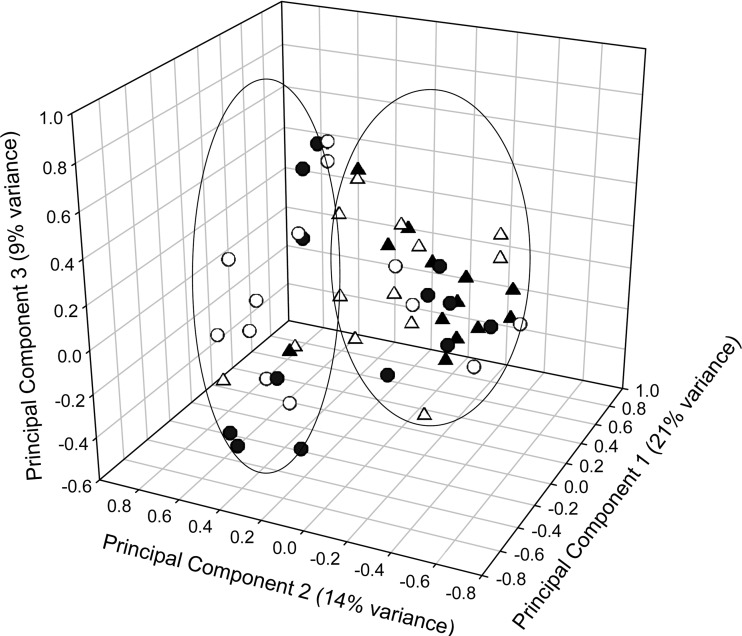
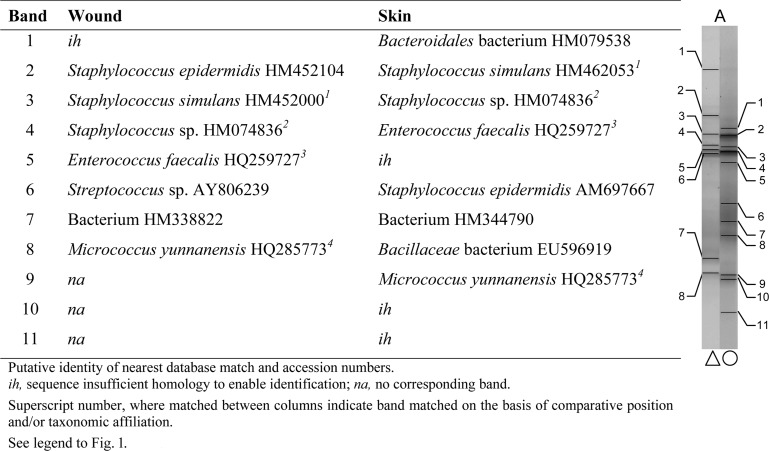
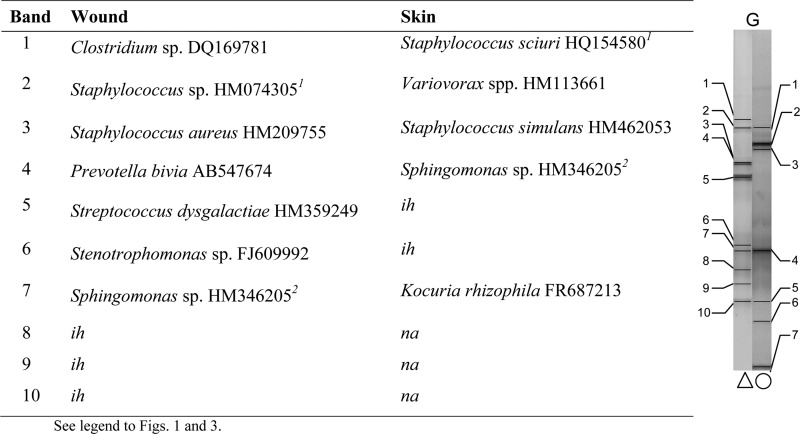
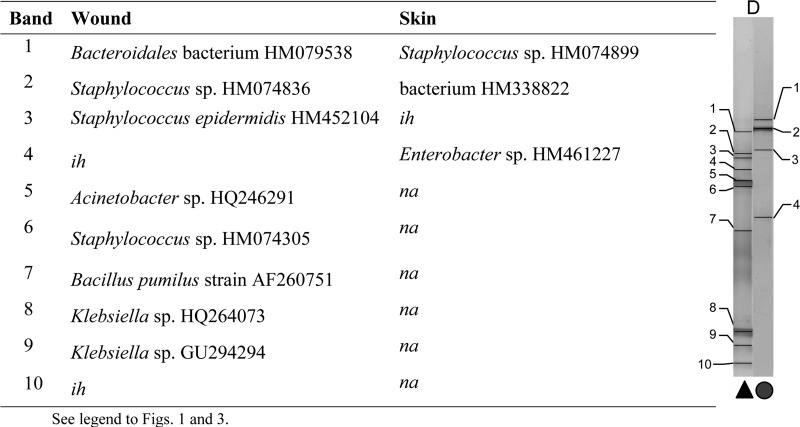
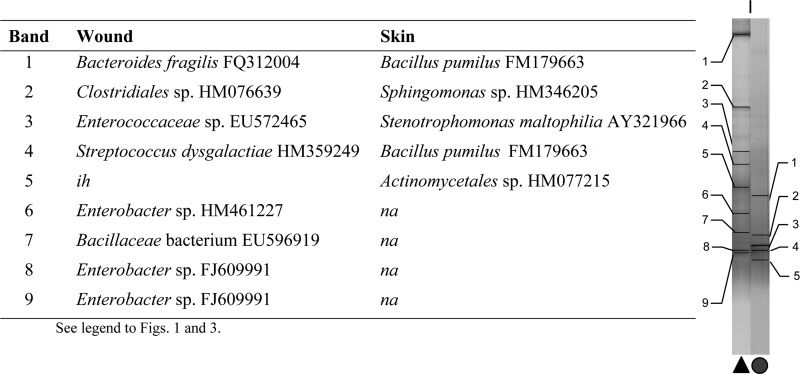
Wound debridement samples and contralateral (healthy) skin swabs acquired from 26 patients attending a specialist foot clinic were analyzed by differential isolation and eubacterium-specific PCR-denaturing gradient gel electrophoresis (DGGE) in conjunction with DNA sequencing. Thirteen of 26 wounds harbored pathogens according to culture analyses, with Staphylococcus aureus being the most common (13/13). Candida (1/13), pseudomonas (1/13), and streptococcus (7/13) were less prevalent. Contralateral skin was associated with comparatively low densities of bacteria, and overt pathogens were not detected. According to DGGE analyses, all wounds contained significantly greater eubacterial diversity than contralateral skin (P < 0.05), although no significant difference in total eubacterial diversity was detected between wounds from which known pathogens had been isolated and those that were putatively uninfected. DGGE amplicons with homology to Staphylococcus sp. (8/13) and S. aureus (2/13) were detected in putatively infected wound samples, while Staphylococcus sp. amplicons were detected in 11/13 noninfected wounds; S. aureus was not detected in these samples. While a majority of skin-derived DGGE consortial fingerprints could be differentiated from wound profiles through principal component analysis (PCA), a large minority could not. Furthermore, wounds from which pathogens had been isolated could not be distinguished from putatively uninfected wounds on this basis. In conclusion, while chronic wounds generally harbored greater eubacterial diversity than healthy skin, the isolation of known pathogens was not associated with qualitatively distinct consortial profiles or otherwise altered diversity. The data generated support the utility of both culture and DGGE for the microbial characterization of chronic wounds.
Figures
References
-
- Bass MJ, Phillips LG. 2007. Pressure sores. Curr. Probl. Surg. 44:101–143 - PubMed
-
- Bourke WJ, O'Connor CM, FitzGerald MX, McDonnell TJ. 1994. Pseudomonas aeruginosa exotoxin A induces pulmonary endothelial cytotoxicity: protection by dibutyryl-cAMP. Eur. Respir. J. 7:1754–1758 - PubMed
-
- Brook I, Frazier EH. 1990. Aerobic and anaerobic bacteriology of wounds and cutaneous abscesses. Arch. Surg. 125:1445–1451 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
