

Surgical outcome of 21 patients with congenital upper eyelid coloboma
- PMID: 22553521
- PMCID: PMC3340657
- DOI: 10.3980/j.issn.2222-3959.2010.01.16
Surgical outcome of 21 patients with congenital upper eyelid coloboma
Abstract
Aim: To evaluate the surgical outcome of congenital upper eyelid coloboma repair.
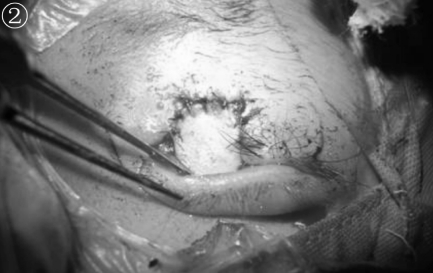
Methods: All patients underwent complete ophthalmic and general examination before going to surgery, and then examination under anesthesia was performed to assess the site and size of eyelid defect, conjunctival involvement. The status of cornea and ocular motility with forced duction test was also being noted. The surgical procedure was performed according to the size of defect.
Results: Out of 21 cases of congenital upper eyelid coloboma, 18 occurred in isolation with upper eyelid medial defect, 13 were bilateral and 5 were unilateral. Others were associated with Goldenhar syndrome and CHARGE syndrome with bilateral upper lid medial defects. All patients were presented for surgical corrections during age of 2.5-4.0 years except one that presented at 25 years of age. Cosmetically surgical results were acceptable, except one that was already presented with opaque corneal.
Conclusion: In this study, overall surgical results were satisfactory except one that was presented late with compromised cornea.
Keywords: coloboma; surgical outcome; upperlid congenital.
Figures







Similar articles
-
Optic Nerve Coloboma.2023 Jun 26. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2023 Jun 26. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30422472 Free Books & Documents.
-
Congenital upper eyelid coloboma with ipsilateral eyebrow hypoplasia.Vojnosanit Pregl. 2012 Sep;69(9):809-11. Vojnosanit Pregl. 2012. PMID: 23050409
-
One-stage reconstruction technique for large congenital eyelid coloboma.Orbit. 2011 Aug;30(4):177-9. doi: 10.3109/01676830.2011.582979. Orbit. 2011. PMID: 21780928
-
Congenital upper eyelid coloboma: embryologic, nomenclatorial, nosologic, etiologic, pathogenetic, epidemiologic, clinical, and management perspectives.Ophthalmic Plast Reconstr Surg. 2015 Jan-Feb;31(1):1-12. doi: 10.1097/IOP.0000000000000347. Ophthalmic Plast Reconstr Surg. 2015. PMID: 25419956 Free PMC article. Review.
-
Adnexal surgery in dogs and cats.Vet Ophthalmol. 2004 Sep-Oct;7(5):284-90. doi: 10.1111/j.1463-5224.2004.04044.x. Vet Ophthalmol. 2004. PMID: 15310287 Review.
Cited by
-
A 5-day-old-newborn with a large right upper eyelid coloboma.Digit J Ophthalmol. 2017 Sep 28;23(3):88-91. doi: 10.5693/djo.03.2017.08.001. eCollection 2017. Digit J Ophthalmol. 2017. PMID: 29162995 Free PMC article. No abstract available.
-
The incidence, embryology, and oculofacial abnormalities associated with eyelid colobomas.Eye (Lond). 2015 Apr;29(4):492-8. doi: 10.1038/eye.2014.335. Epub 2015 Jan 23. Eye (Lond). 2015. PMID: 25613848 Free PMC article.
-
Manifestation and grading of ocular involvement in patients with Tessier number 10 clefts.Eye (Lond). 2017 Aug;31(8):1140-1145. doi: 10.1038/eye.2017.39. Epub 2017 Mar 17. Eye (Lond). 2017. PMID: 28304389 Free PMC article.
-
Case report: A novel intronic JMJD6 likely pathogenic variant (c.941+75G > T) associated with congenital eyelid coloboma in one of the identical twin sisters.Front Genet. 2025 Feb 17;16:1536000. doi: 10.3389/fgene.2025.1536000. eCollection 2025. Front Genet. 2025. PMID: 40034743 Free PMC article.
-
Congenital Upper Eyelid Coloboma: Clinical and Surgical Management.Case Rep Ophthalmol Med. 2015;2015:286782. doi: 10.1155/2015/286782. Epub 2015 Aug 23. Case Rep Ophthalmol Med. 2015. PMID: 26366313 Free PMC article.
References
-
- Pagon RA. Ocular coloboma. Surv Ophthalmol. 1981;25(4):223–236. - PubMed
-
- Seath LL, Choo CT, Fong KS. Congenital upper lid colobomas management and visual outcome. Ophthal Plast Reconstr Surg. 2002;18(3):190–195. - PubMed
-
- Tessier P. Symposium on Plastic Surgery in the Orbital Region. St. Louis: CV Mosby; 1980. Anatomical classification of facial, cranoi-facial and latero facial clefts.
-
- Roper Hall MJ. Proceedings of the Second International Symposium in Plastic and Reconstructive Surgery of the Eye and Adnexa. St. Louis: CV Mosby; 1967. Congenital coloboma of the lids; pp. 316–321.
-
- Duke-Elder S, Cook C. Normal and abnormal development. In: Duke-Elder S, editor. System of Ophthalmology. Vol. 14. St. Louis: C.V. Mosby Co; 1963. pp. 313–317.
LinkOut - more resources
Full Text Sources