

Plasma expander and blood storage effects on capillary perfusion in transfusion after hemorrhage
- PMID: 22554380
- PMCID: PMC4517570
- DOI: 10.1111/j.1537-2995.2012.03679.x
Plasma expander and blood storage effects on capillary perfusion in transfusion after hemorrhage
Abstract
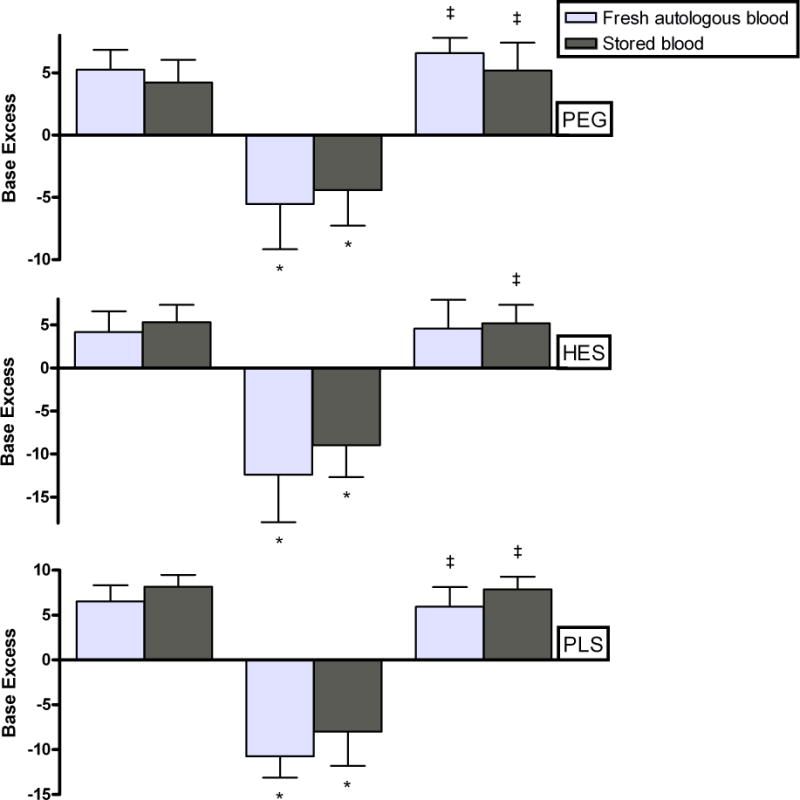
Background: Treating hemorrhage with blood transfusions in subjects previously hemodiluted with different colloidal plasma expanders, using fresh autologous blood or blood that has been stored for 2 weeks, allows identifying the interaction between type of plasma expander and differences in blood storage.
Study design and methods: Studies used the hamster window chamber model. Fresh autologous plasma, 130-kDa starch-based plasma expander (hydroxyethyl starch [HES]), or 4% polyethylene glycol-conjugated albumin (PEG-Alb) was used for 20% of blood volume (BV) hemodilution. Hemodilution was followed by a 55% by BV 40-minute hemorrhagic shock period, treated with transfusion of fresh or blood that was stored for 2 weeks. Outcome was evaluated 1 hour after blood transfusion in terms of microvascular and systemic variables.
Results: Results were principally dependent on the type of colloidal solution used during hemodilution, 4% PEG-Alb yielding the best microvascular recovery evaluated in terms of the functional capillary density. This result was consistent whether fresh blood or stored blood was used in treating the subsequent shock period. Fresh blood results were significantly better in systemic and microvascular terms relative to stored blood. HES and fresh plasma hemodilution yielded less favorable results, a difference that was enhanced when fresh versus stored blood was compared in their efficacy of correcting the subsequent hemorrhage.
Conclusion: The type of plasma expander used for hemodilution influences the short-term outcome of subsequent volume resuscitation using blood transfusion, 4% PEG-Alb providing the most favorable outcome by comparison to HES or fresh plasma.
© 2012 American Association of Blood Banks.
Conflict of interest statement
Figures







Similar articles
-
Survival time in severe hemorrhagic shock after perioperative hemodilution is longer with PEG-conjugated human serum albumin than with HES 130/0.4: a microvascular perspective.Crit Care. 2008;12(2):R54. doi: 10.1186/cc6874. Epub 2008 Apr 18. Crit Care. 2008. PMID: 18423033 Free PMC article.
-
Effects on cardiac function of a novel low viscosity plasma expander based on polyethylene glycol conjugated albumin.Minerva Anestesiol. 2011 Jul;77(7):704-14. Minerva Anestesiol. 2011. PMID: 21709658
-
Early difference in tissue pH and microvascular hemodynamics in hemorrhagic shock resuscitation using polyethylene glycol-albumin- and hydroxyethyl starch-based plasma expanders.Shock. 2005 Jul;24(1):66-73. doi: 10.1097/01.shk.0000167111.80753.ef. Shock. 2005. PMID: 15988323
-
Microcirculatory effects of intravenous fluids in critical illness: plasma expansion beyond crystalloids and colloids.Curr Opin Anaesthesiol. 2009 Apr;22(2):163-7. doi: 10.1097/ACO.0b013e328328d304. Curr Opin Anaesthesiol. 2009. PMID: 19307891 Review.
-
Warm fresh whole blood transfusion for severe hemorrhage: U.S. military and potential civilian applications.Crit Care Med. 2008 Jul;36(7 Suppl):S340-5. doi: 10.1097/CCM.0b013e31817e2ef9. Crit Care Med. 2008. PMID: 18594261 Review.
Cited by
-
The ebb and flow of fluid (as in resuscitation).Eur J Trauma Emerg Surg. 2015 Apr;41(2):119-27. doi: 10.1007/s00068-014-0437-0. Epub 2014 Aug 20. Eur J Trauma Emerg Surg. 2015. PMID: 26038255 Review.
References
-
- Tsai AG, Cabrales P, Acharya SA, Intaglietta M. Resuscitation from hemorrhagic shock: recovery of oxygen carrying capacity or perfusion? Efficacy of new plasma expanders. Transfusion Alternatives in Transfusion Medicine. 2007;9:246–53.
-
- Tsai AG, Intaglietta M. High viscosity plasma expanders: Volume restitution fluids for lowering the transfusion trigger. Biorheology. 2001;38:229–37. - PubMed
-
- Schou H, Kongstad L, Perez de Sa V, Werner O, Larsson A. Uncompensated blood loss is not tolerated during acute normovolemic hemodilution in anesthetized pigs. Anesth Analg. 1998;87:786–94. - PubMed
-
- Van der Linden P, Gilbart E, Paques P, Simon C, Vincent JL. Influence of hematocrit on tissue O2 extraction capabilities during acute hemorrhage. Am J Physiol. 1993;264:H1942–7. - PubMed
-
- Van der Linden P, Vincent JL. Normovolemic hemodilution and acute hemorrhage. Anesth Analg. 1999;89:532–3. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
