

Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results
- PMID: 22555112
- PMCID: PMC3389193
- DOI: 10.1016/j.ophtha.2012.03.053
Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration: two-year results
Abstract
Objective: To describe effects of ranibizumab and bevacizumab when administered monthly or as needed for 2 years and to describe the impact of switching to as-needed treatment after 1 year of monthly treatment.
Design: Multicenter, randomized clinical trial.
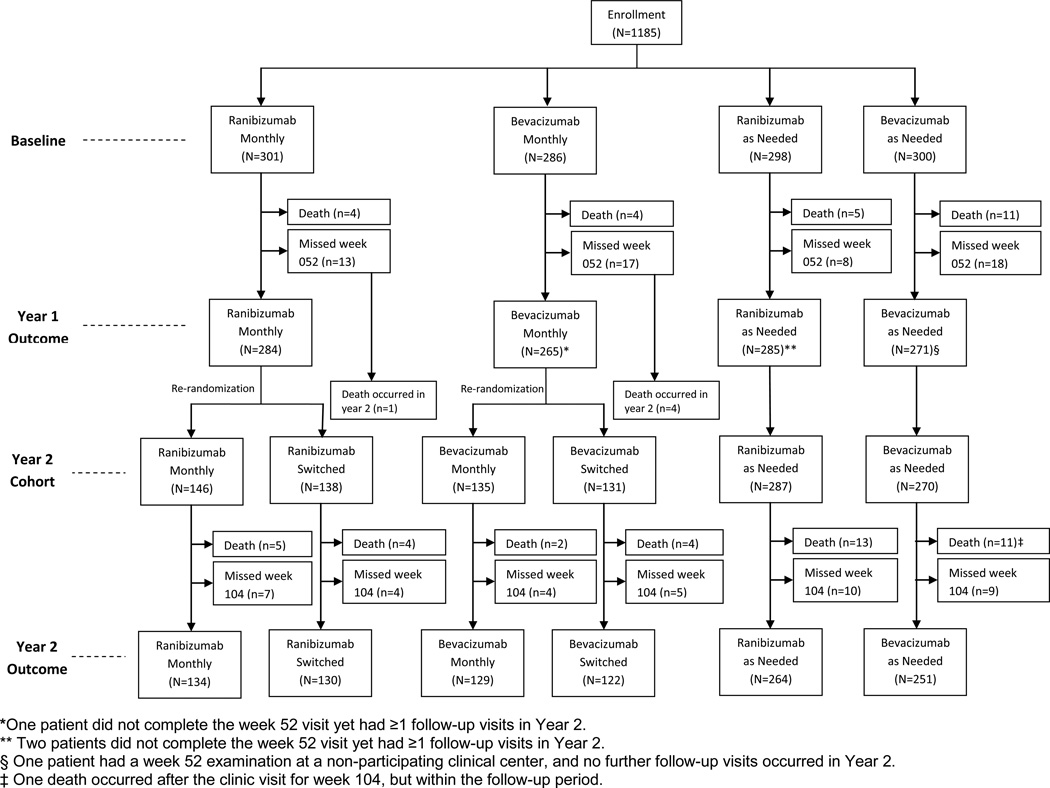
Participants: Patients (n = 1107) who were followed up during year 2 among 1185 patients with neovascular age-related macular degeneration who were enrolled in the clinical trial.
Interventions: At enrollment, patients were assigned to 4 treatment groups defined by drug (ranibizumab or bevacizumab) and dosing regimen (monthly or as needed). At 1 year, patients initially assigned to monthly treatment were reassigned randomly to monthly or as-needed treatment, without changing the drug assignment.
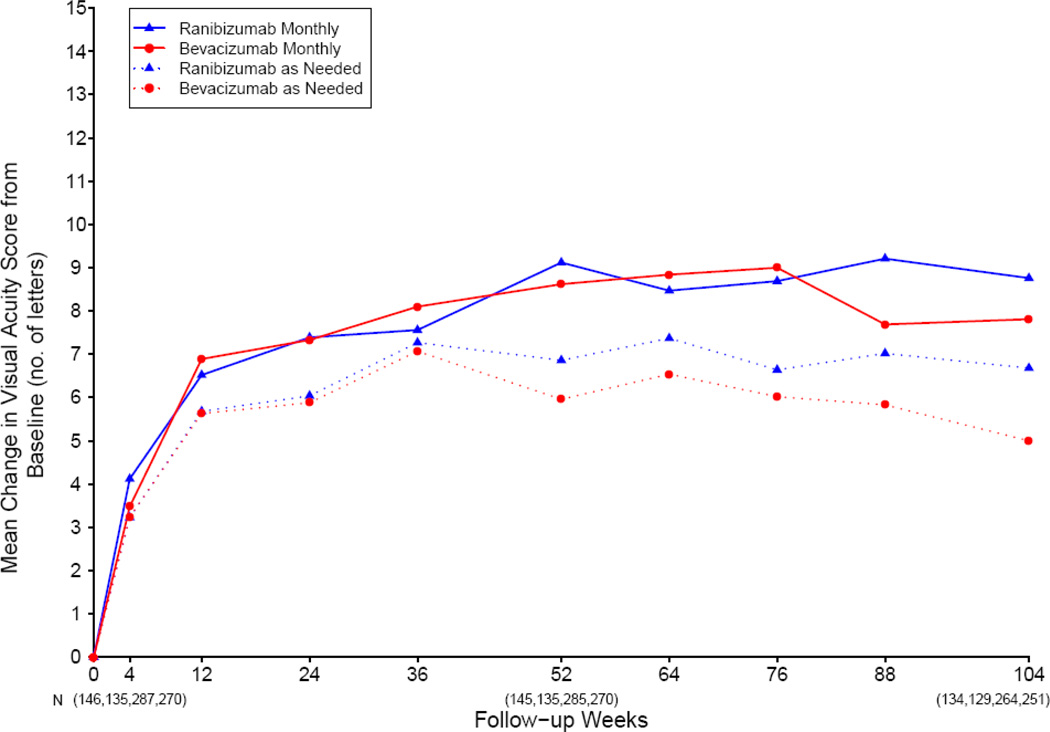
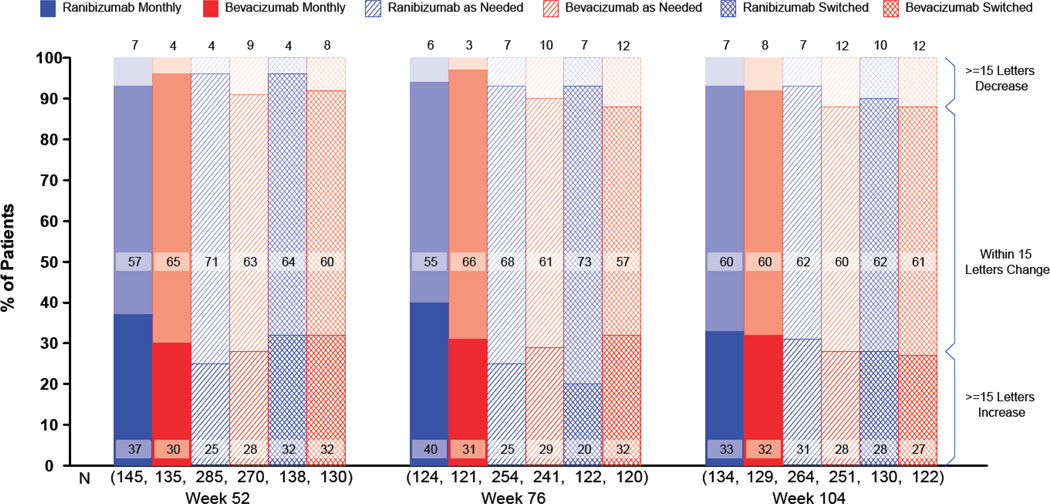
Main outcome measures: Mean change in visual acuity.
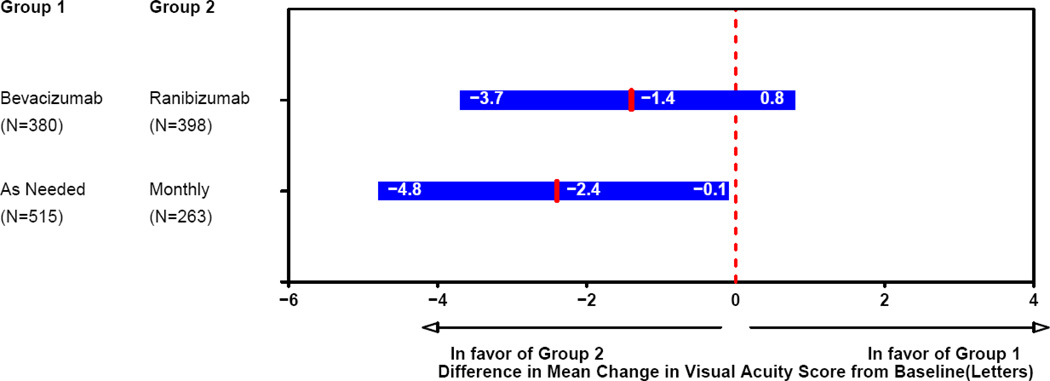
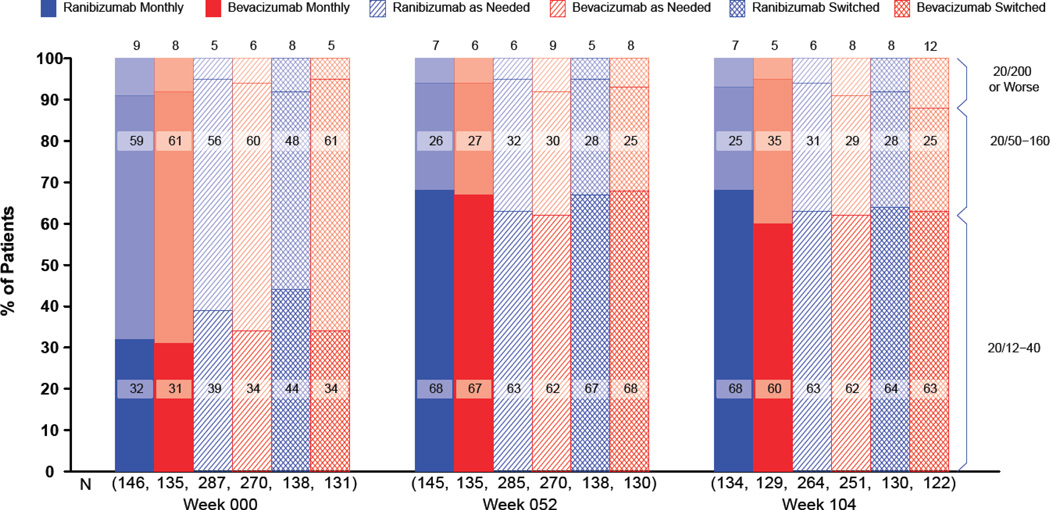
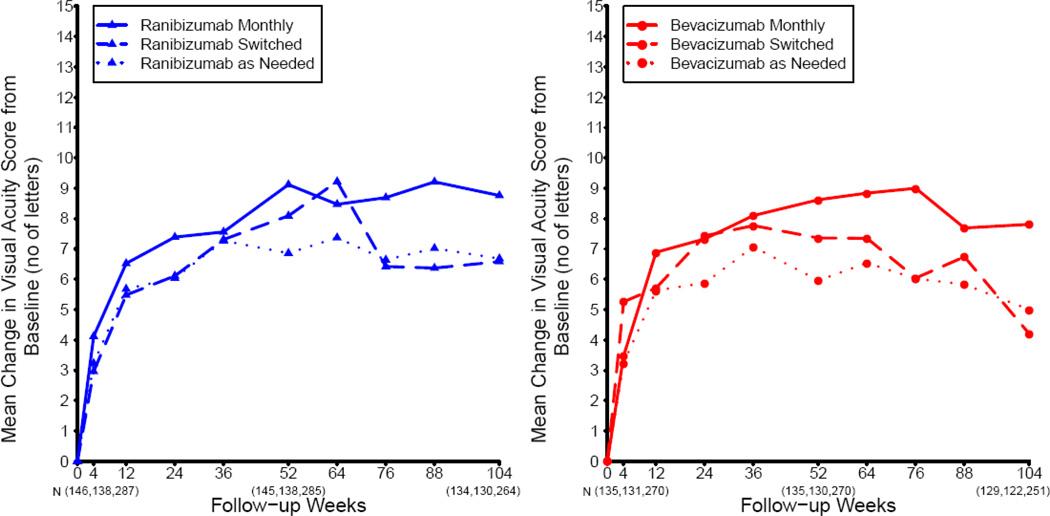
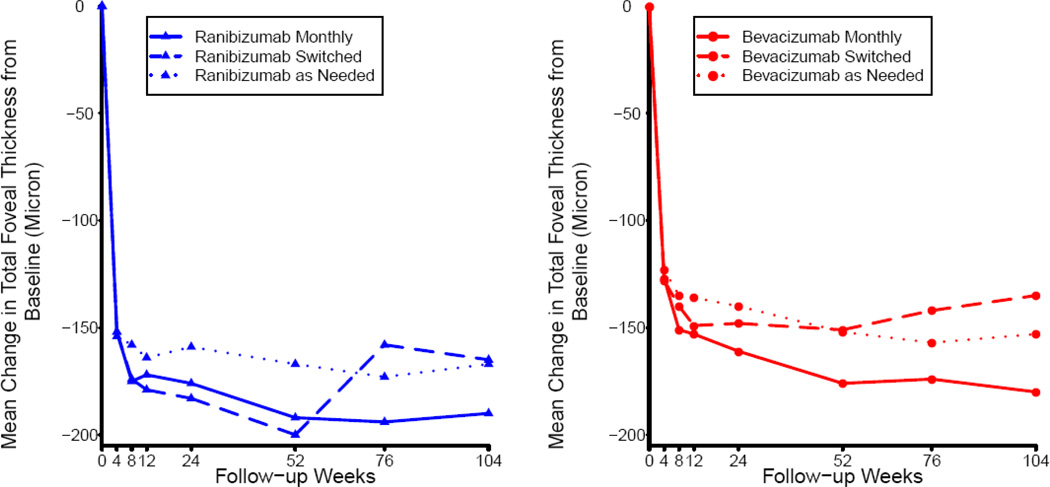
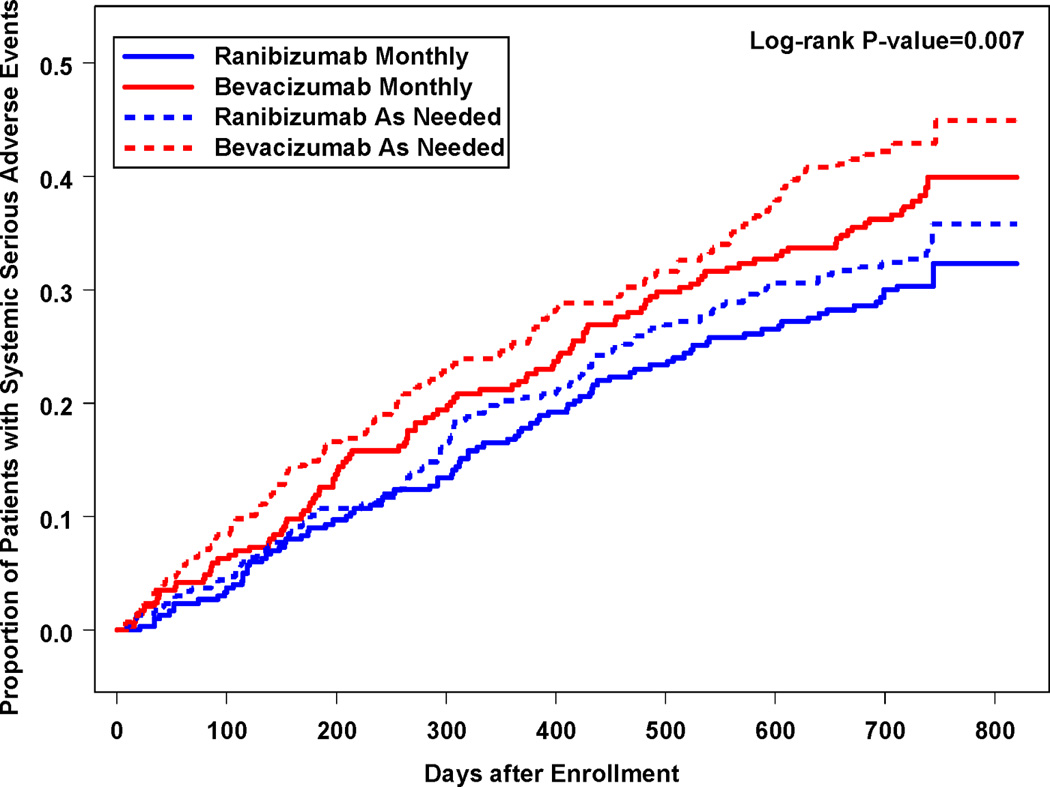
Results: Among patients following the same regimen for 2 years, mean gain in visual acuity was similar for both drugs (bevacizumab-ranibizumab difference, -1.4 letters; 95% confidence interval [CI], -3.7 to 0.8; P = 0.21). Mean gain was greater for monthly than for as-needed treatment (difference, -2.4 letters; 95% CI, -4.8 to -0.1; P = 0.046). The proportion without fluid ranged from 13.9% in the bevacizumab-as-needed group to 45.5% in the ranibizumab monthly group (drug, P = 0.0003; regimen, P < 0.0001). Switching from monthly to as-needed treatment resulted in greater mean decrease in vision during year 2 (-2.2 letters; P = 0.03) and a lower proportion without fluid (-19%; P < 0.0001). Rates of death and arteriothrombotic events were similar for both drugs (P > 0.60). The proportion of patients with 1 or more systemic serious adverse events was higher with bevacizumab than ranibizumab (39.9% vs. 31.7%; adjusted risk ratio, 1.30; 95% CI, 1.07-1.57; P = 0.009). Most of the excess events have not been associated previously with systemic therapy targeting vascular endothelial growth factor (VEGF).
Conclusions: Ranibizumab and bevacizumab had similar effects on visual acuity over a 2-year period. Treatment as needed resulted in less gain in visual acuity, whether instituted at enrollment or after 1 year of monthly treatment. There were no differences between drugs in rates of death or arteriothrombotic events. The interpretation of the persistence of higher rates of serious adverse events with bevacizumab is uncertain because of the lack of specificity to conditions associated with inhibition of VEGF.
Copyright © 2012 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Anti-VEGF therapies for the treatment of age-related macular degeneration.J Comp Eff Res. 2012 Nov;1(6):485-8. doi: 10.2217/cer.12.57. J Comp Eff Res. 2012. PMID: 24236467
-
Comparative effectiveness of bevacizumab and ranibizumab in the comparison of age-related macular degeneration treatments trials.JAMA Ophthalmol. 2015 Mar;133(3):363-4. doi: 10.1001/jamaophthalmol.2014.4642. JAMA Ophthalmol. 2015. PMID: 25429419 No abstract available.
-
Analyses Comparing Visual Acuity Between Ranibizumab and Bevacizumab in the Comparison of Age-Related Macular Degeneration Treatments Trials.JAMA Ophthalmol. 2015 Jun;133(6):726. doi: 10.1001/jamaophthalmol.2015.0502. JAMA Ophthalmol. 2015. PMID: 25811288 Free PMC article. No abstract available.
References
-
- Brown DM, Kaiser PK, Michels M, et al. ANCHOR Study Group. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355:1432–1444. - PubMed
-
- Rosenfeld PJ, Brown DM, Heier JS, et al. MARINA Study Group. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355:1419–1431. - PubMed
-
- Brechner RJ, Rosenfeld PJ, Babish JD, Caplan S. Pharmacotherapy for neovascular age-related macular degeneration: an analysis of the 100% 2008 Medicare fee-for-service Part B claims file. Am J Ophthalmol. 2011;151:887–895. - PubMed
-
- Office of the Inspector General, Department of Health and Human Services. Review of Medicare Part B Avastin and Lucentis treatments for age-related macular degeneration (A-01-10-00514) [letter] [Accessed February 16, 2012];2011 Sep; Available at: http://oig.hhs.gov/oas/reports/region10/11000514.pdf.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
