

Prevention of invasive cervical cancer in the United States: past, present, and future
- PMID: 22556273
- PMCID: PMC3556792
- DOI: 10.1158/1055-9965.EPI-11-1158
Prevention of invasive cervical cancer in the United States: past, present, and future
Abstract
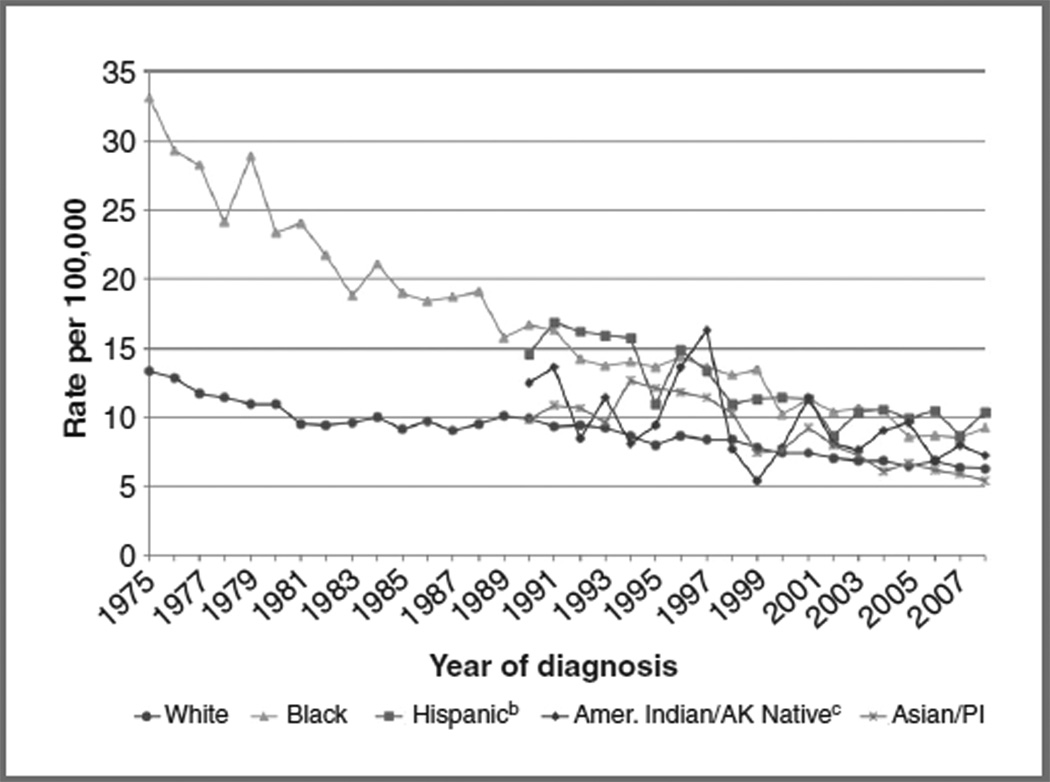
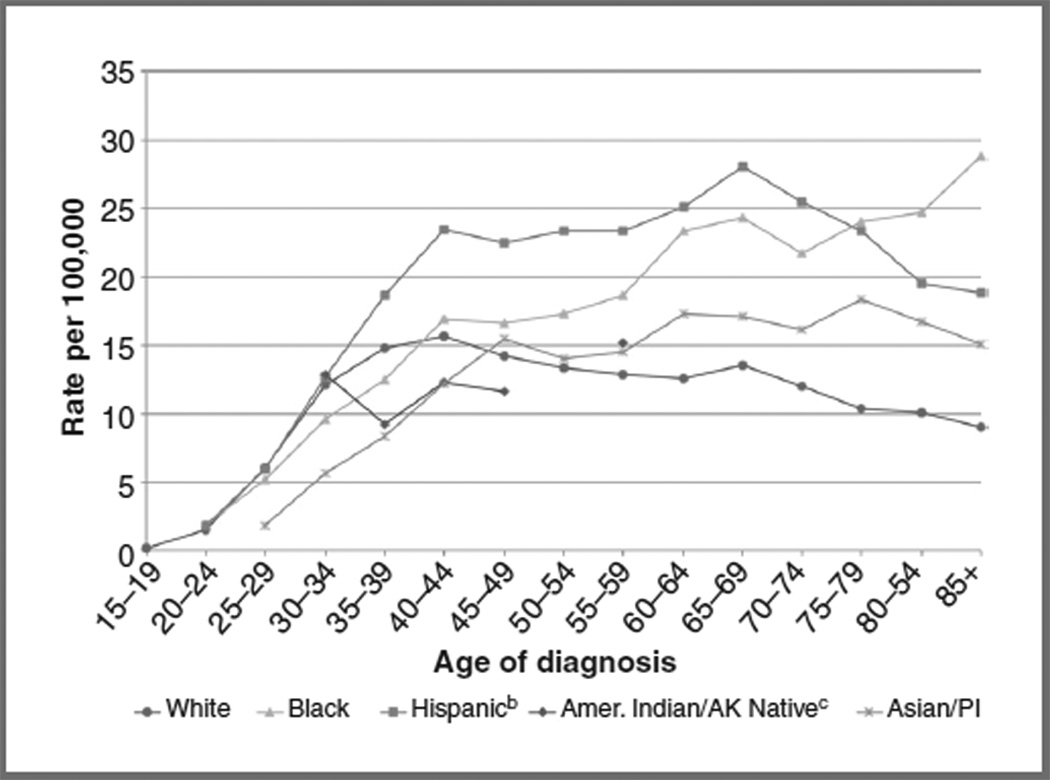
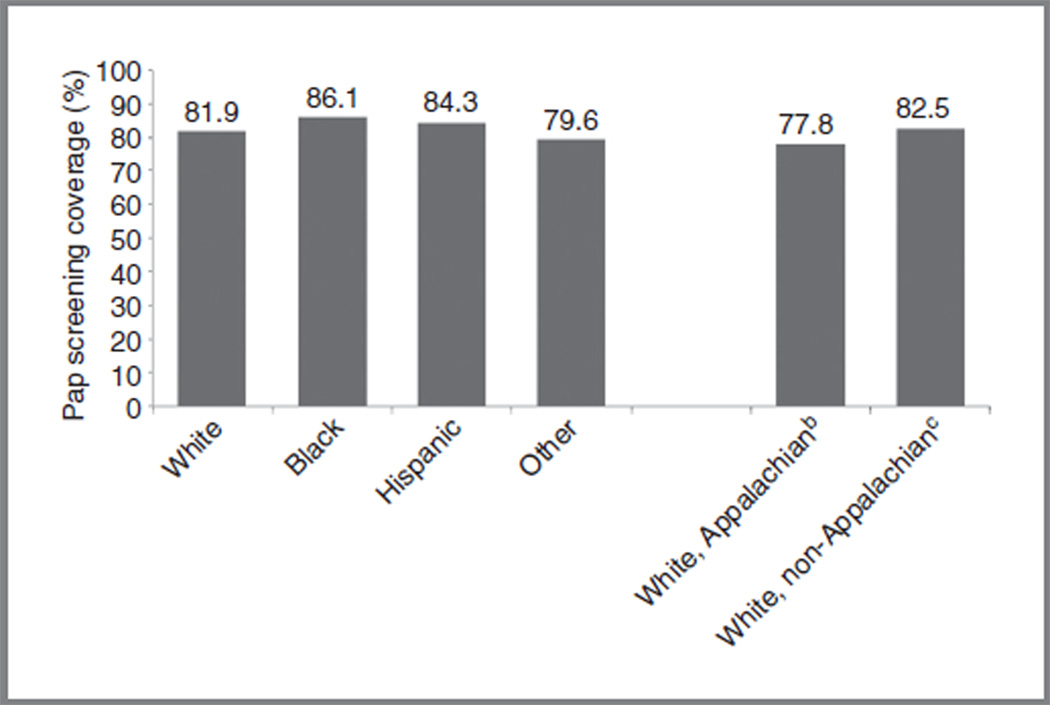
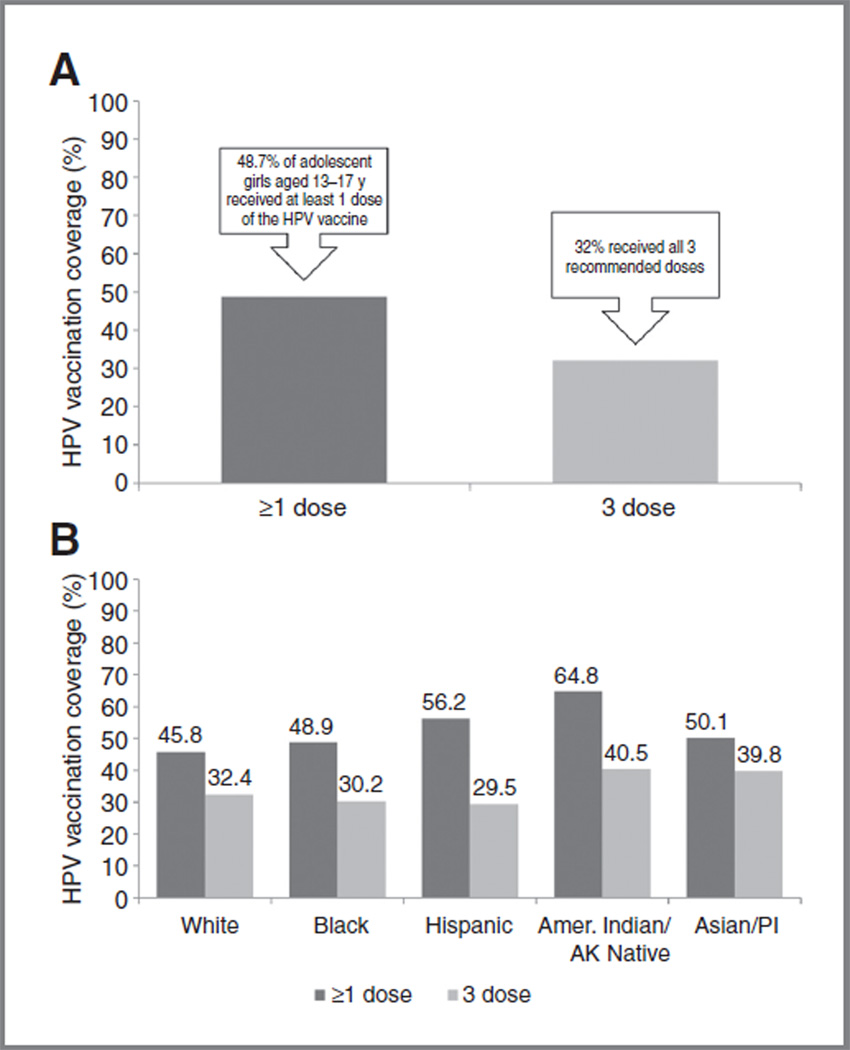
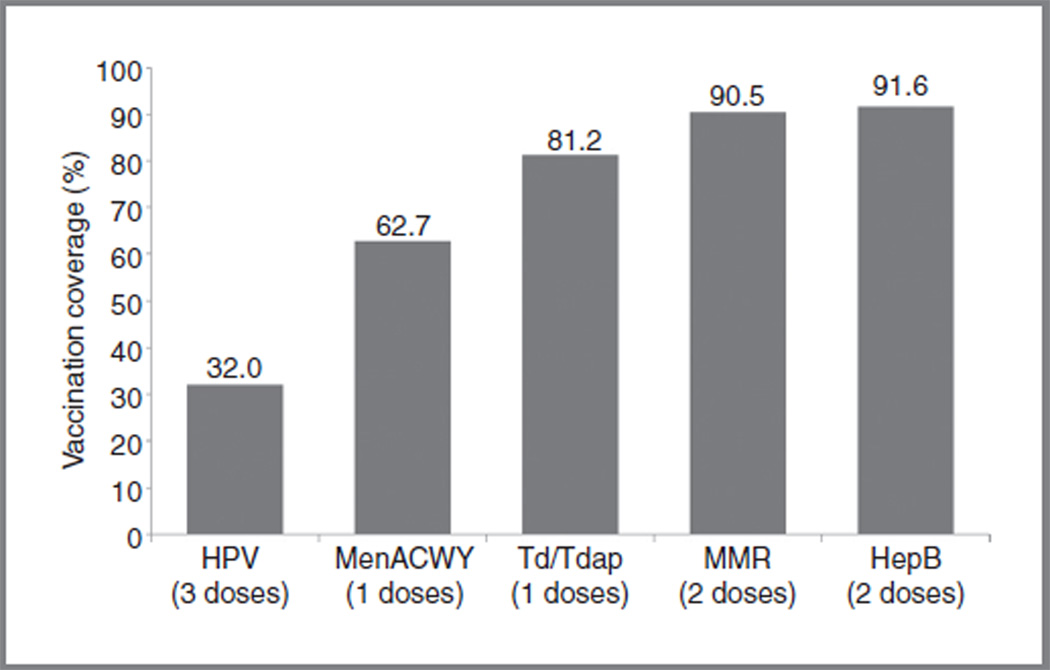
Over the past several decades, invasive cervical cancer (ICC) incidence in the United States has declined dramatically. Much of this decline has been attributed to widespread use of cytology screening followed by treatment of precancerous lesions. Despite available technologies to prevent ICC and screening programs targeting high-risk women, certain populations in the United States experience disproportionately high rates of ICC (e.g., racial/ethnic minorities and rural women). Limited access to and use of screening/follow-up services underlie this disparity. The licensure of the human papillomavirus (HPV) vaccine in 2006 introduced an additional method of ICC prevention. Unfortunately, dissemination of the vaccine to age-eligible females has been lower than expected (32% have received all 3 recommended doses). Decreasing the burden of HPV infection and HPV-related diseases in the United States will require greater dissemination of the HPV vaccine to adolescents and young adults, along with successful implementation of revised ICC screening guidelines that incorporate HPV and cytology cotesting. While a future without ICC is possible, we will need a comprehensive national health care program and innovative approaches to reduce ICC burden and disparities.
©2012 AACR
Conflict of interest statement
E.D. Paskett received commercial research support from Merck. A.R. Giuliano received a commercial research grant from Merck and commercial research support from GSK. A.R. Giuliano received an honoraria from Speaker’s bureau and is a consultant/advisory board member in Merck. No potential conflicts of interest were disclosed by the other authors.
Figures
References
-
- American Cancer Society. Cancer facts & figures 2011. Atlanta, GA: American Cancer Society; 2011.
-
- Howlader N, Noone A, Krapcho M, Neyman N, Aminou R, Waldron W, et al. SEER cancer statistics review, 1975–2008. Bethesda, MD: National Cancer Institute; 2011. [cited 2011 Nov 29]. Available from: http://seer.cancer.gov/csr/1975_2008.
-
- Patel NR, Rollison DE, Barnholtz-Sloan J, Mackinnon J, Green L, Giuliano AR. Racial and ethnic disparities in the incidence of invasive cervical cancer in Florida. Cancer. 2009;115:3991–4000. - PubMed
