

Usefulness of blood supply visualization by indocyanine green fluorescence for reconstruction during esophagectomy
- PMID: 22557942
- PMCID: PMC3339581
- DOI: 10.1007/s10388-011-0291-7
Usefulness of blood supply visualization by indocyanine green fluorescence for reconstruction during esophagectomy
Abstract
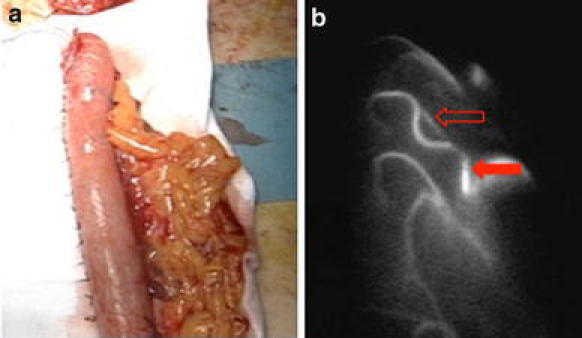
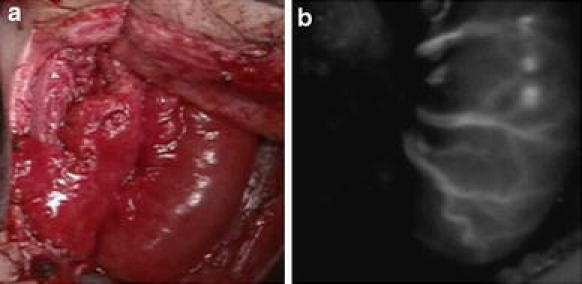
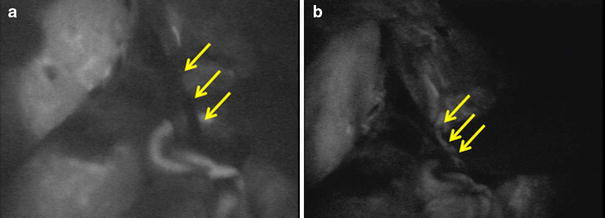
BACKGROUND: Adequate blood supply for the reconstructed organ is important for safe esophagogastric anastomosis during esophagectomy. Recently, indocyanine green (ICG) has been used for visualization of the blood supply when anastomosis is performed in vascular surgery. To visualize the blood supply for reconstruction, we employed ICG fluorescence during esophagectomy. METHODS: From August 2008, 40 patients received cervical or thoracic esophagectomy. They consisted of 33 patients having esophagectomy for thoracic esophageal cancer, 3 being treated for cervical esophageal cancer, and 4 with double cancer of the thoracic and cervical regions. Before and after pulling up the reconstructed organ, 2.5 mg of ICG was injected as a bolus. Then ICG fluorescence was detected by a camera and recorded. RESULTS: ICG fluorescence was easily detected in all patients at 1 min after injection. The vascular network was well visualized in the gastric wall, colonic grafts, and free jejunal grafts. In five patients, we also performed anastomosis between the short gastric vein and the external cervical vein or superficial cervical vein. The intraoperative and postoperative course of all patients was uneventful apart from three anastomotic leakages. CONCLUSIONS: ICG fluorescence can be employed to evaluate the blood supply to reconstructed organs and can be useful in selecting the patients who do not need additional vessel anastomosis. However, anastomotic leakage was not reduced, so the microcirculation detected by ICG fluorescence did not necessarily provide appropriate blood supply for a viable anastomosis.
Figures



References
-
- Alanezi K, Urschel JD. Mortality secondary to esophageal anastomotic leak. Ann Thorac Cardiovasc Surg. 2004;10:71–75. - PubMed
LinkOut - more resources
Full Text Sources