

Combined use of EUS-guided FNA and immunocytochemical stains discloses metastatic and unusual diseases in the evaluation of mediastinal lymphadenopathy of unknown etiology
- PMID: 22558013
- PMCID: PMC3339209
- DOI: 10.4103/1817-1737.94527
Combined use of EUS-guided FNA and immunocytochemical stains discloses metastatic and unusual diseases in the evaluation of mediastinal lymphadenopathy of unknown etiology
Abstract
Purpose: Mediastinal lymphadenopathy (ML) is a cause for concern, especially in patients with previous malignancy. We report our experience with the use of endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) with immunocytochemical stains in patients being evaluated for ML.
Methods: Retrospective analysis of patients with ML of unknown origin who underwent EUS-FNA. On-site evaluation was performed by experienced cytologist, and special immunocytochemical stains were requested as indicated.
Results: A total of 116 patients were included, and a total of 136 mediastinal LN were sampled. Prior malignancy was present in 45%. The most common site of examined lymph node (LN) were subcarinal (76%, 103 LN). The median long and short axis diameters were 28 mm and 13 mm, respectively. FNA was read on-site as malignant, 21 (16%); benign, 100 (76.9%); suspicious, six (4%); atypical, 3 (2%); and inadequate sample, six (4%). Sixty-four LN were deferred for additional studies; 22 for immunocytochemical and 26 for Gimesa (GMS) stain and 21 for flow cytometry. Final FNA read was malignant in 28 (21%), benign in 103 (76%), suspicious in three (2%), and atypical in two (1%). Metastatic malignancies disclosed included Hodgkin's and Non-Hodgkin's lymphoma, melanoma, hepatoma, breast, lung, colon, renal, endometrial, Fallopian tube, and unknown carcinoma. The sensitivity, specificity, and accuracy of the final FNA read to predict malignancy were 100%.
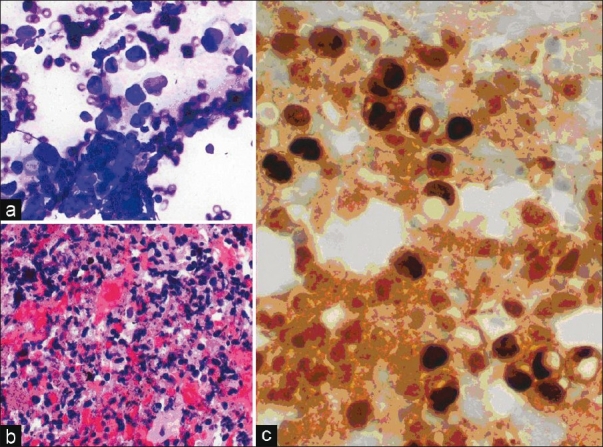
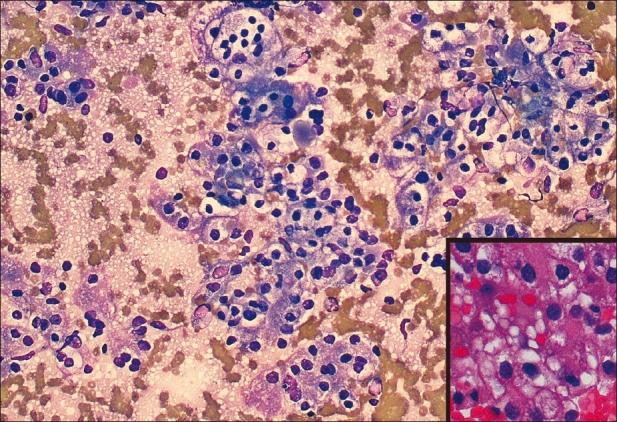
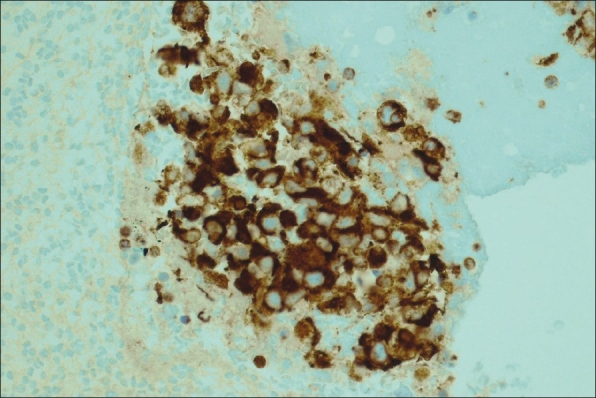
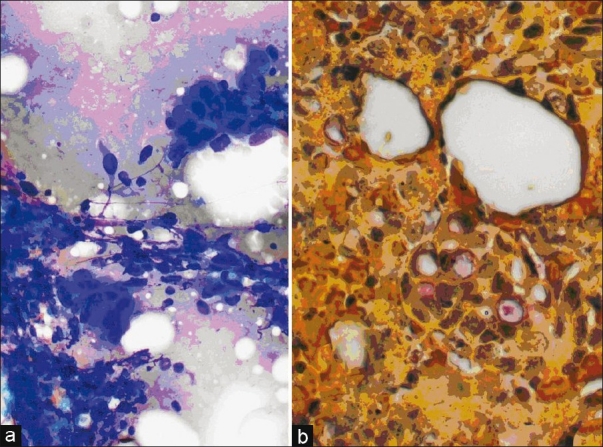
Conclusion: EUS-guided FNA with additional ancillary studies is useful in disclosing metastatic ML from a variety of neoplasms. Due to its safety and accuracy profile, it should be considered the test of choice in evaluating abnormal ML in appropriately selected patients.
Keywords: Endoscopic ultrasound; fine needle aspiration; immunostains; lung cancer; metastatic disease.
Conflict of interest statement
Figures
References
-
- Geisinger KR. Differential diagnostic considerations and potential pitfalls in fine-needle aspiration biopsies of the mediastinum. Diagn Cytopathol. 1995;13:436–42. - PubMed
-
- Cerfolio RJ, Bryant AS, Ojha B, Eloubeidi M. Improving the inaccuracies of clinical staging of patients with NSCLC: A prospective trial. Ann Thorac Surg. 2005;80:1207–14. - PubMed
-
- Wiersema MJ, Kochman ML, Chak A, Cramer HM, Kesler KA. Real time endoscopic ultrasound guided fine needle aspiration of mediastinal lymph node. Gastrointest Endosc. 1993;39:429–31. - PubMed
-
- Klapman JB, Logrono R, Dye CE, Waxman I. Clinical impact of on-site cytopathology interpretation on endoscopic ultrasound-guided fine needle aspiration. Am J Gastroenterol. 2003;98:1289–94. - PubMed
-
- Singh HK, Silverman JF, Powers CN, Geisinger KR, Frable WJ. Diagnostic pitfalls in fine-needle aspiration biopsy of the mediastinum. Diagn Cytopathol. 1997;17:121–6. - PubMed
LinkOut - more resources
Full Text Sources
Medical
