

Obstructed labor and caesarean delivery: the cost and benefit of surgical intervention
- PMID: 22558089
- PMCID: PMC3338803
- DOI: 10.1371/journal.pone.0034595
Obstructed labor and caesarean delivery: the cost and benefit of surgical intervention
Abstract
Background: Although advances in the reduction of maternal mortality have been made, up to 273,000 women will die this year from obstetric etiologies. Obstructed labor (OL), most commonly treated with Caesarean delivery, has been identified as a major contributor to global maternal morbidity and mortality. We used economic and epidemiological modeling to estimate the cost per disability-adjusted life-year (DALY) averted and benefit-cost ratio of treating OL with Caesarean delivery for 49 countries identified as providing an insufficient number of Caesarean deliveries to meet demand.
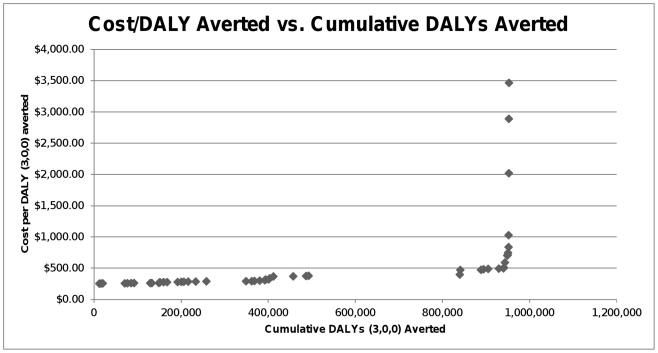
Methods and findings: Using publicly available data and explicit economic assumptions, we estimated that the cost per DALY (3,0,0) averted for providing Caesarean delivery for OL ranged widely, from $251 per DALY averted in Madagascar to $3,462 in Oman. The median cost per DALY averted was $304. Benefit-cost ratios also varied, from 0.6 in Zimbabwe to 69.9 in Gabon. The median benefit-cost ratio calculated was 6.0. The main limitation of this study is an assumption that lack of surgical capacity is the main factor responsible for DALYs from OL.
Conclusions: Using the World Health Organization's cost-effectiveness standards, investing in Caesarean delivery can be considered "highly cost-effective" for 48 of the 49 countries included in this study. Furthermore, in 46 of the 49 included countries, the benefit-cost ratio was greater than 1.0, implying that investment in Caesarean delivery is a viable economic proposition. While Caesarean delivery alone is not sufficient for combating OL, it is necessary, cost-effective by WHO standards, and ultimately economically favorable in the vast majority of countries included in this study.
Conflict of interest statement
Figures
References
-
- Lozano R, Wang H, Foreman KJ, Rajaratnam JK, Naghavi M, et al. Progress towards Millennium Development Goals 4 and 5 on maternal and child mortality: an updated systematic analysis. Lancet. 2011;378:1139–1165. - PubMed
-
- Graham WJ, Cairns J, Bhattacharya S, Bullough CH, Quayyum Z, et al. Maternal and Perinatal Conditions. Disease Control Priorities in Developing Countries (2nd Edition) New York: Oxford University Press; 2006. pp. 499–530.
-
- World Health Organization, UNICEF, UNFPA, The World Bank. Trends in maternal mortality: 1990 to 2008 – Estimates developed by WHO, UNICEF, UNFPA and The World Bank. Geneva, Switzerland: World Health Organization; 2010. 45
-
- Khan KS, Wojdyla D, Say L, Gulmezoglu AM, Van Look PF. WHO analysis of causes of maternal death: a systematic review. Lancet. 2006;367:1066–1074. - PubMed
-
- Dolea C, AbouZahr C. Global Burden of obstructed labor in the year 2000: version 2. Geneva: WHO; 2003.
