Laparoscopic assisted central pancreatectomy with pancreaticogastrostomy reconstruction - An alternative surgical technique for central pancreatic mass resection
- PMID: 22558594
- PMCID: PMC3339104
- DOI: 10.4297/najms.2010.2438
Laparoscopic assisted central pancreatectomy with pancreaticogastrostomy reconstruction - An alternative surgical technique for central pancreatic mass resection
Abstract
Context: Central pancreatectomy has gained popularity in the past decade as treatment of choice for low malignant potential tumor in the midpancreas due to its ability to achieve optimal preservation of pancreatic parenchyma. Simultaneously, advancement in minimally invasive approach has contributed to numerous novel surgical techniques with significantly lower morbidity and mortality. With the purpose of improving patient outcomes, we describe a laparoscopic assisted central pancreatectomy with pancreaticogastrostomy as an alternative method to the previously described open central pancreatectomy with roux-en-y pancreaticojejunostomy reconstruction.
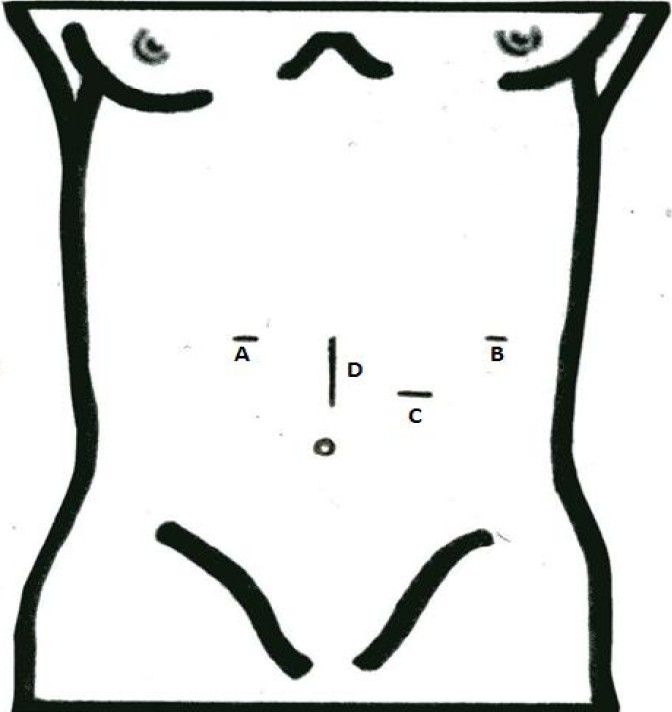
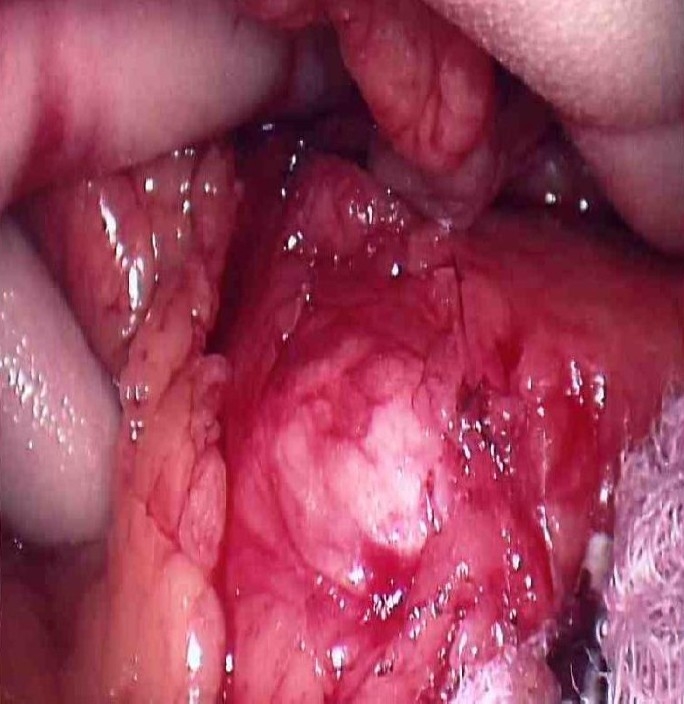
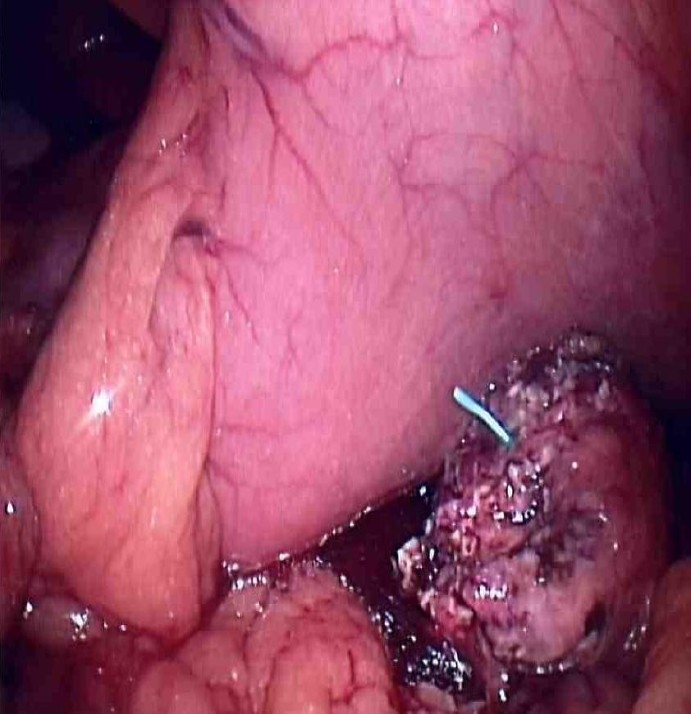
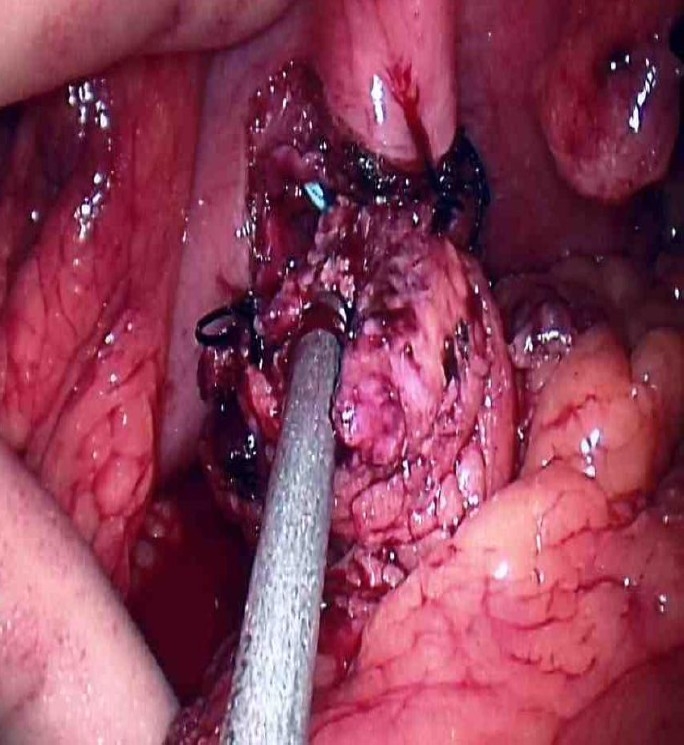
Case report: A 39 year old man presented to our clinic with a 2.5 cm neuroendocrine tumor at the neck of the pancreas. Laparoscopic assisted central pancreatectomy with pancreaticogastrostomy reconstruction was successfully performed. Operative time was 210 minutes with blood loss of 200 ml. Postoperative course was uneventful except for a minimal pancreatic leak which was controlled by an intraoperatively placed closed suction drain. At 2 week follow up, patient was asymptomatic with well preserved pancreatic endo and exocrine functions. Permanent pathology findings showed a well differentiated neuroendocrine tumor with negative margins and nodes.
Conclusions: Laparoscopic assisted central pancreatectomy with pancreaticogastrostomy reconstruction is feasible and safe for a centrally located tumor. Laparoscopic assisted technique facilitates application of minimally invasive approach by increasing surgical feasibility in typically complex pancreatic operations.
Keywords: Laparoscopic; central pancreatectomy; pancreaticogastrostomy.
Figures
References
-
- Owen NJ, Sohaid SA, Peppercorn PD, et al. MRI of neuroendocrine pancreatic tumors. Br J Radiol. 2001;74:968–973. - PubMed
-
- Van NY, Vandaele S, Opde BB, et al. Neuroendocrine tumors of the pancreas: benefits of new technologies. Surg Endosc. 2003;17:1658–1662. - PubMed
-
- Christein JD, Kim AW, Goldshan MA, et al. Central pancreatectomy for the resection of benign or low malignant potential neoplasm. World J Surg. 2003;27(5):595–598. - PubMed
-
- Takada T, Yasuda H, Uchiyama K, et al. Pancreatic enzyme activity after pylorus-preserving pancreaticoduodenectomy reconstructed with pancreaticogastrostomy. Pancreas. 1995;11:276–282. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous