

Preoperative treatment planning with intraoperative optimization can achieve consistent high-quality implants in prostate brachytherapy
- PMID: 22560295
- PMCID: PMC3935513
- DOI: 10.1016/j.meddos.2012.03.001
Preoperative treatment planning with intraoperative optimization can achieve consistent high-quality implants in prostate brachytherapy
Abstract
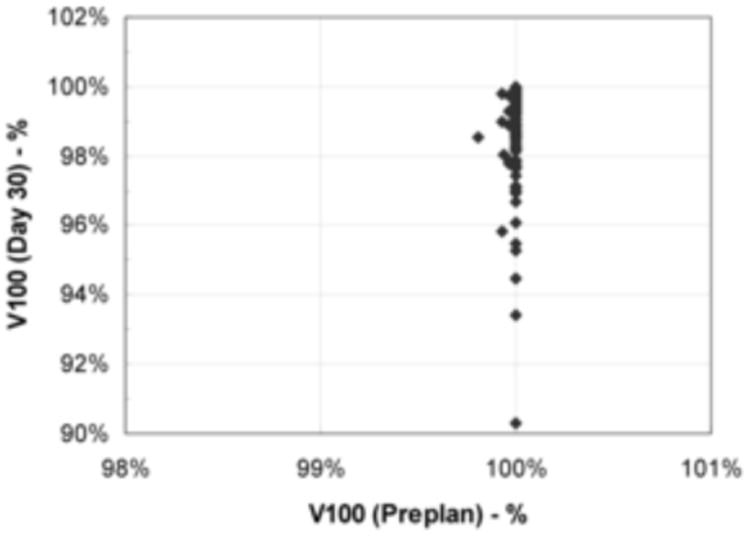
Advances in brachytherapy treatment planning systems have allowed the opportunity for brachytherapy to be planned intraoperatively as well as preoperatively. The relative advantages and disadvantages of each approach have been the subject of extensive debate, and some contend that the intraoperative approach is vital to the delivery of optimal therapy. The purpose of this study was to determine whether high-quality permanent prostate implants can be achieved consistently using a preoperative planning approach that allows for, but does not necessitate, intraoperative optimization. To achieve this purpose, we reviewed the records of 100 men with intermediate-risk prostate cancer who had been prospectively treated with brachytherapy monotherapy between 2006 and 2009 at our institution. All patients were treated with iodine-125 stranded seeds; the planned target dose was 145 Gy. Only 8 patients required adjustments to the plan on the basis of intraoperative findings. Consistency and quality were assessed by calculating the correlation coefficient between the planned and implanted amounts of radioactivity and by examining the mean values of the dosimetric parameters obtained on preoperative and 30 days postoperative treatment planning. The amount of radioactivity implanted was essentially identical to that planned (mean planned radioactivity, 41.27 U vs. mean delivered radioactivity, 41.36 U; R(2) = 0.99). The mean planned and day 30 prostate V100 values were 99.9% and 98.6%, respectively. The mean planned and day 30 prostate D90 values were 186.3 and 185.1 Gy, respectively. Consistent, high-quality prostate brachytherapy treatment plans can be achieved using a preoperative planning approach, mostly without the need for intraoperative optimization. Good quality assurance measures during simulation, treatment planning, implantation, and postimplant evaluation are paramount for achieving a high level of quality and consistency.
Copyright © 2012. Published by Elsevier Inc.
Conflict of interest statement
Figures


References
-
- Potters L, Klein EA, Kattan MW, et al. Monotherapy for stage T1-T2 prostate cancer: radical prostatectomy, external beam radiotherapy, or permanent seed implantation. Radiother Oncol. 2004;71:29–33. - PubMed
-
- Stone NN, Hong S, Lo YC, et al. Comparison of intraoperative dosimetric implant representation with postimplant dosimetry in patients receiving prostate brachytherapy. Brachytherapy. 2003;2:17–25. - PubMed
-
- Ishiyama H, Nakamura R, Satoh T, et al. Differences between intraoperative ultrasound-based dosimetry and postoperative computed tomography-based dosimetry for permanent interstitial prostate brachytherapy. Brachytherapy. 2010;9:219–23. - PubMed
-
- Zelefsky MJ, Zaider M. Low-dose-rate brachytherapy for prostate cancer: preplanning vs. intraoperative planning-intraoperative planning is best. Brachytherapy. 2006;5:143–4. - PubMed
-
- Blasko JC. Low-dose-rate brachytherapy for prostate cancer: preplanning vs. intraoperative planning-preplanning is best. Brachytherapy. 2006;5:139–42. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
